


Stool tests serve as a vital biochemical screening tool in the United Kingdom for detecting microscopic amounts of blood that may indicate the presence of colon polyps or certain complications related to diverticular disease. While these tests cannot directly visualise the structure of the bowel or provide a definitive diagnosis of a specific condition, they identify patients who require further investigation, such as a colonoscopy or CT scan. The primary test used within the national health framework is the Faecal Immunochemical Test, which is designed to find hidden blood that is not visible to the naked eye. Because polyps and inflamed diverticular pouches can both bleed intermittently, the presence of human haemoglobin in a stool sample acts as a clinical marker for structural abnormalities. In the UK, these tests are a cornerstone of preventative medicine, allowing for the early detection of issues before they progress or cause significant physical symptoms. Understanding the role and limitations of stool testing is essential for patients participating in national screening programmes or undergoing diagnostic reviews for bowel habit changes. By utilising these non-invasive tools, the healthcare system can prioritise those at highest risk and ensure that resources are directed toward definitive diagnostic procedures when biochemical indicators suggest an underlying bowel concern.
What We’ll Discuss in This Article
- The function of the Faecal Immunochemical Test in detecting hidden blood.
- How microscopic bleeding links to the presence of colon polyps.
- The role of stool tests in identifying symptomatic diverticular disease.
- Differentiating between screening results and a definitive clinical diagnosis.
- Why certain stool tests are used to rule out inflammatory bowel conditions.
- UK clinical pathways for following up on abnormal stool test results.
The Role of the Faecal Immunochemical Test (FIT)
The Faecal Immunochemical Test is the primary stool test used in the United Kingdom to detect microscopic traces of blood, which can suggest the presence of polyps even when an individual feels perfectly healthy. Polyps are small growths on the inner lining of the large intestine that have a delicate surface and a rich blood supply. The NHS states that the FIT kit is the main test used in the bowel cancer screening programme to look for tiny amounts of blood in your poo that you cannot see.
As waste passes through the colon, it can cause minor abrasions on a polyp, leading to the release of blood into the stool. The FIT kit is highly specific to human haemoglobin, meaning it is not affected by diet or medication, making it a reliable biochemical indicator. In the UK, this test is used to screen the asymptomatic population within specific age groups. While a positive result does not confirm a polyp is present, it indicates that the bowel lining requires a visual inspection, typically via a colonoscopy, to find the source of the bleeding. This proactive approach ensures that polyps are identified and removed while they are small, maintaining the long-term health of the colon mucosa.
Stool Tests and Diverticular Disease Indicators
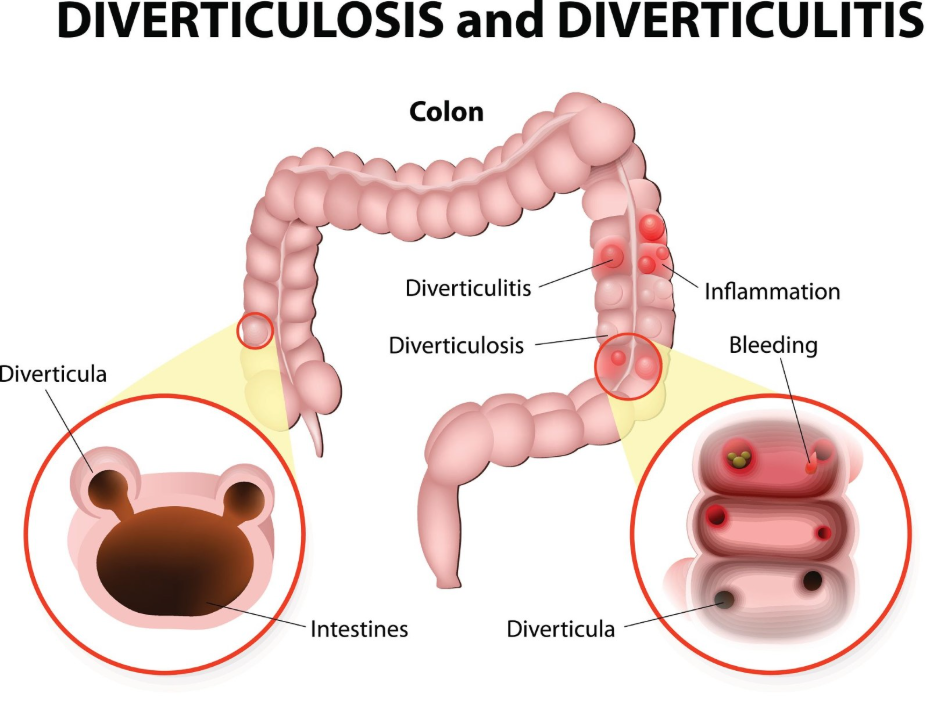
While stool tests are not typically used to diagnose uncomplicated diverticulosis, they can suggest the presence of diverticular disease if the pouches are inflamed or bleeding. Diverticula are small pockets that bulge outward from the colon wall; when these become irritated, they can shed blood in a similar way to polyps. NICE clinical guidelines for diverticular disease management indicate that a stool test may be used to look for occult blood or to rule out other causes of abdominal symptoms.
In cases of early or mild diverticulitis, the inflammation may cause the bowel lining to become reactive and bleed slightly. A stool test can detect this blood, helping clinicians determine if a patient’s discomfort is related to a structural bowel issue rather than a functional problem like Irritable Bowel Syndrome. However, for a patient experiencing an acute flare-up with severe pain and fever, UK clinicians usually prioritise imaging like a CT scan over stool tests. The stool test is most valuable in the “sub-acute” or chronic phase, where it helps monitor the stability of the bowel and ensures that persistent bleeding is not overlooked.
Differentiating Between Screening and Diagnosis
It is important to understand that a stool test is a screening tool that suggests a potential issue, rather than a diagnostic test that confirms exactly what is happening in the colon. An abnormal result indicates that blood was found, but it cannot tell the difference between blood from a polyp, an inflamed diverticulum, or a common issue like haemorrhoids.
| Test Aspect | Stool Test (FIT) | Visual Test (Colonoscopy) |
| Primary Goal | Screening for hidden blood. | Direct diagnosis and removal of growths. |
| Invasiveness | Non-invasive home kit. | Invasive hospital procedure. |
| Result Type | Biochemical (Yes/No for blood). | Visual (Direct view of lining). |
| Actionable Step | Triggers further investigation. | Allows for immediate treatment (polypectomy). |
In the United Kingdom, the clinical pathway always moves from the stool test to a more definitive investigation if blood is detected. This staged approach ensures that only those with a measurable biochemical marker undergo invasive procedures. For patients with diverticular disease, the stool test provides a way to monitor for complications without the need for frequent scans. By using the stool test as a “first filter,” the UK healthcare system can manage a large population effectively, ensuring that the structural and cellular health of the colon is monitored through the most appropriate clinical tools.
Ruling Out Other Inflammatory Conditions
In addition to looking for blood, certain stool tests measure proteins like calprotectin to help clinicians determine if symptoms are caused by inflammation, such as in early diverticulitis or inflammatory bowel disease. Faecal calprotectin is a marker released by white blood cells when they move into the intestinal lining to fight infection or inflammation.
NICE clinical guidelines for investigating gastrointestinal symptoms suggest that faecal calprotectin testing can help distinguish between non-inflammatory conditions and those that involve active bowel inflammation. If a patient has abdominal pain or a change in bowel habits, a low calprotectin level might suggest that diverticulitis is not currently active. A high level, however, indicates that the bowel is inflamed and requires further investigation. This test is particularly useful in the UK for helping GPs decide whether a patient needs an urgent referral to a gastroenterologist. While it does not specifically find polyps, it is a vital tool for assessing the general inflammatory status of the colon wall and lining.
UK Clinical Pathways for Abnormal Results
The management of an abnormal stool test result in the United Kingdom involves a structured follow-up process designed to identify the source of the bleeding or inflammation promptly. If a national screening FIT kit returns an abnormal result, the individual is typically referred to a specialist centre for a colonoscopy. This is because a visual check is the only way to definitively rule out polyps or confirm diverticular disease as the source of the blood.
For those experiencing symptoms, the GP will use the stool test results alongside a physical examination and medical history. The GOV.UK health pages indicate that integrated diagnostic pathways ensure that patients with abnormal stool markers receive timely access to the most appropriate secondary investigations. If diverticular disease is confirmed during the follow-up, the focus shifts to dietary management. If polyps are found, they are usually removed during the procedure. This coordinated care ensures that no structural abnormalities are missed and that the patient receives a comprehensive assessment of their bowel health, regardless of whether the initial test was triggered by a routine screening or a clinical concern.
Limitations of Stool Testing in Bowel Health
While stool tests are highly effective, they have limitations, such as the fact that they can only detect polyps or diverticulitis if they are actively bleeding at the time the sample is taken. Some polyps bleed only intermittently, meaning a single stool test could theoretically return a “normal” result even if a growth is present. This is why the UK screening programme repeats the test every two years for eligible adults.
Furthermore, stool tests cannot detect polyps that do not bleed at all, which is why clinical symptoms like a persistent change in bowel habits should always be reported to a doctor, regardless of a recent stool test result. In diverticular disease, a stool test may be normal even if a person has many pouches, provided those pouches are not currently inflamed. Understanding these limitations helps patients recognise that a stool test is one part of a wider diagnostic toolkit. In the UK, healthcare providers emphasise that while a “normal” result is reassuring, it must be balanced with self-awareness of any new or worsening gastrointestinal symptoms.
Conclusion
Stool tests such as the FIT kit are essential for detecting hidden blood that may suggest the presence of colon polyps or inflamed diverticula. While these tests provide a valuable biochemical signal, they are screening tools that require follow-up with visual investigations to reach a definitive diagnosis. In the UK, these tests allow for the prioritisation of patients who need a colonoscopy to have polyps removed or diverticular disease managed. Participating in regular screening and reporting any changes in bowel habits are the most effective ways to maintain colon health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a stool test tell the difference between a polyp and diverticulitis?
No; the test only detects the presence of blood or inflammation markers and cannot identify the specific cause; a colonoscopy or scan is needed for that.
Why do I need a colonoscopy if my stool test was only slightly abnormal?
Even a small amount of hidden blood can be a sign of a polyp that needs to be removed before it grows or changes further.
Can eating certain foods affect my FIT test result?
No; the FIT kit used in the UK is specific to human blood and is not affected by food, unlike older versions of stool tests.
If my stool test is normal, does it mean I have no diverticula?
Not necessarily; you can have diverticula (pouches) that are not bleeding or inflamed, which would result in a normal stool test.
How often should I do a stool test if I have a history of polyps?
You should follow the specific surveillance schedule given by your hospital, which usually involves regular colonoscopies rather than just stool tests.
Does a stool test find all types of polyps?
The test only finds polyps that are bleeding; some polyps do not bleed, which is why repeat screening and symptom awareness are important.
What is the calprotectin test used for?
This specific stool test measures inflammation and helps doctors distinguish between functional issues like IBS and inflammatory issues like diverticulitis.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the use of stool tests for polyps and diverticulitis, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with extensive experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


