What role do obesity and lack of exercise play in coronary artery disease?
Obesity and physical inactivity are often grouped together as lifestyle risks, but they attack the heart in distinct, powerful ways. It is not simply a matter of carrying extra weight; excess fat tissue is biologically active, releasing harmful chemicals that damage blood vessels. Similarly, lack of exercise deprives the heart of the conditioning it needs to pump efficiently. Understanding the biological mechanisms behind these factors is the first step toward reclaiming you1r heart health.
What We’ll Discuss in This Article
- How excess body fat acts as an active organ that damages the heart.
- The specific danger of visceral (belly) fat compared to general weight.
- How a sedentary lifestyle lowers ‘good’ cholesterol and weakens the heart.
- The cluster of risks known as Metabolic Syndrome.
- The physiological benefits of regular movement for artery health.
- Differentiating between ‘fat but fit’ and true cardiovascular risk.
- Practical steps to reverse risk through lifestyle changes.
How does obesity directly damage the coronary arteries?
Obesity damages coronary arteries primarily through chronic inflammation and increased cardiac workload. Excess fat tissue, particularly visceral fat around the abdomen, releases inflammatory chemicals (cytokines) that injure the lining of the blood vessels. This accelerates the buildup of plaque (atherosclerosis) while simultaneously forcing the heart to pump harder to supply blood to the larger body mass.
The ‘Active’ Fat Danger
Medical consensus now views fat, especially visceral fat, as an active endocrine organ, not just energy storage.
- Inflammation: Visceral fat cells release proteins that cause systemic inflammation, making cholesterol plaque more likely to form and rupture.
- Insulin Resistance: Excess weight often leads to Type 2 diabetes, which significantly damages blood vessels.
- Haemodynamic Strain: The heart must generate higher pressure to push blood through the additional tissue, leading to hypertension and thickening of the heart muscle (hypertrophy).
How does a lack of exercise contribute to blocked arteries?
A sedentary lifestyle contributes to blocked arteries by altering blood chemistry and weakening the heart muscle. Without regular physical activity, levels of ‘good’ (HDL) cholesterol, which scrubs arteries clean, drop significantly. Additionally, the endothelial cells lining the arteries become sluggish and less able to dilate (open up) to accommodate blood flow, leading to higher blood pressure and stiffer vessels.
The ‘Use It or Lose It’ Principle
- Low HDL: Exercise is one of the most effective ways to boost HDL cholesterol. Inactivity allows LDL (bad) cholesterol to linger in the bloodstream.
- Poor Circulation: Regular movement encourages the growth of ‘collateral’ blood vessels, tiny natural bypasses that can help supply the heart if a main artery gets blocked. Sedentary individuals lack this safety net.
- Metabolic Slowdown: Inactivity reduces the body’s ability to process blood sugar and fats, leaving them to accumulate in the vessels.
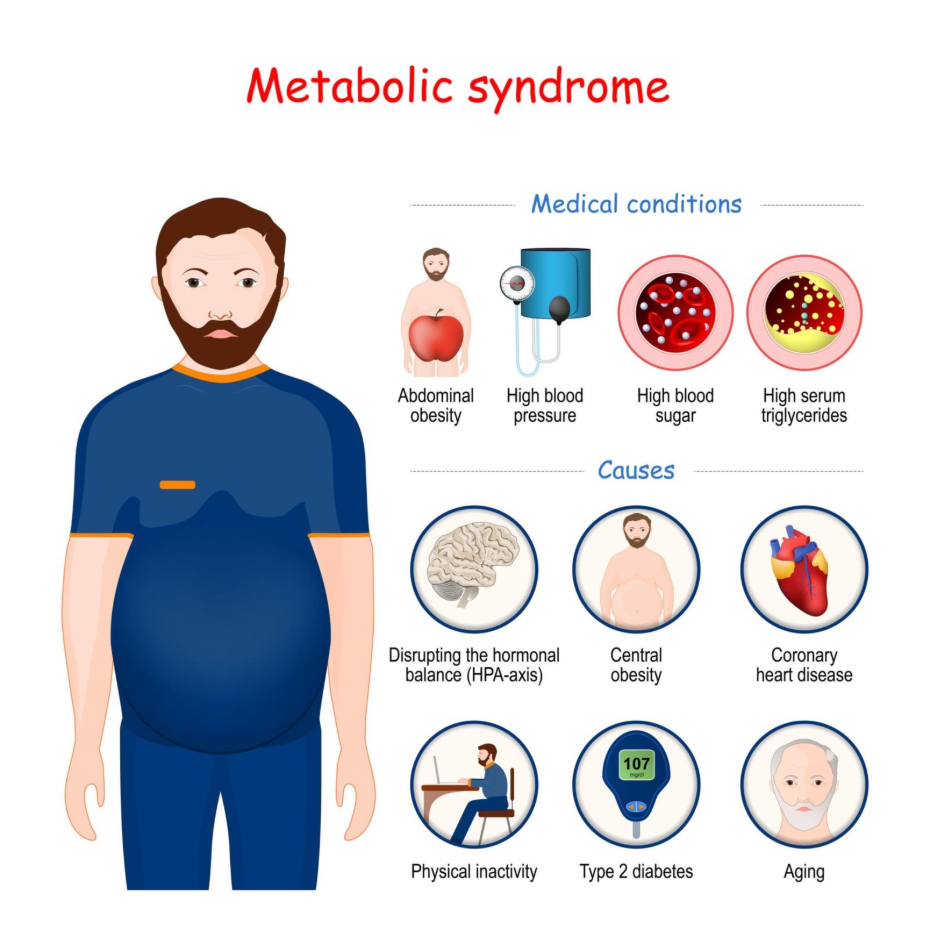
What is ‘Metabolic Syndrome’?
Metabolic syndrome is a dangerous cluster of conditions that occur together, increasing your risk of heart disease, stroke, and type 2 diabetes. It is strongly linked to obesity and inactivity. You are considered to have this syndrome if you have three or more of the following: a large waistline, high triglyceride levels, low HDL cholesterol, high blood pressure, or high fasting blood sugar.
Getty Images
The Multiplier Effect
Having just one of these risk factors is dangerous, but having them in combination (the syndrome) makes you roughly twice as likely to develop heart disease.
- Central Adiposity: Carrying weight around the waist (apple shape) is a stronger predictor of heart attacks than BMI alone.
- Insulin Resistance: The body struggles to use insulin effectively, keeping blood sugar and fat levels high.
Triggers: The Danger of the ‘Weekend Warrior’
For those who are obese and sedentary, sudden intense exercise can be a trigger for a cardiac event. If the arteries are already narrowed by plaque, a sudden demand for high blood flow (e.g., running for a bus or intense shovelling) can cause plaque to rupture or trigger a fatal arrhythmia. This is why ‘start slow’ is medical advice, not just a slogan.
- Plaque Rupture: Mechanical stress from sudden high blood pressure during exertion can tear unstable plaque.
- Supply/Demand Mismatch: The unconditioned heart needs massive amounts of oxygen during stress but cannot get it through narrowed pipes.
Differentiation: BMI vs. Waist Circumference
While Body Mass Index (BMI) is a general measure, waist circumference is a more accurate predictor of coronary artery disease risk. A person can have a ‘normal’ BMI but high visceral fat (thin on the outside, fat on the inside), putting them at high cardiac risk. Conversely, an athlete may have a high BMI due to muscle but low cardiac risk.
- BMI: A rough calculation of weight vs. height.
- Waist Size: A direct measure of visceral fat.
- Risk Thresholds: Men with a waist size above 94cm (37in) and women above 80cm (31.5in) are at increased risk.
Conclusion
Obesity and inactivity are not passive states; they actively drive the biological processes that clog arteries and stress the heart. Visceral fat generates inflammation, while a sedentary life removes the body’s natural defences against cholesterol. However, this risk is reversible. Even losing a small amount of weight (5–10%) and introducing moderate daily walking can drastically reduce the strain on your heart and lower your risk of a future event.
If you experience chest pain, severe breathlessness, or dizziness while exercising, stop immediately. If symptoms do not subside within 15 minutes, call 999.
You may find our free BMI Calculator helpful for understanding or monitoring your symptoms.
Can I be fat and fit?
It is possible to have high cardiovascular fitness while being overweight (‘fat and fit’), which offers some protection. However, the presence of excess body fat still exerts long-term metabolic, inflammatory, and haemodynamic strain on the heart compared to being a healthy weight.
How much exercise do I need to reduce heart risk?
The NHS recommends at least 150 minutes of moderate-intensity activity a week, such as brisk walking, or 75 minutes of vigorous activity.
Does walking count as exercise for the heart?
Yes. Brisk walking is excellent for heart health. It improves circulation, lowers blood pressure, and helps manage weight without placing extreme stress on the joints or heart.
Why is belly fat worse for the heart than thigh fat?
Belly (visceral) fat surrounds your internal organs and is metabolically active, releasing toxins and hormones that raise blood pressure and cholesterol. Thigh (subcutaneous) fat is generally less metabolically harmful.
Is it too late to start exercising if I have heart disease?
No. Exercise is a core part of treatment for diagnosed heart disease (Cardiac Rehabilitation). However, you must consult your doctor before starting to ensure the intensity is safe for your specific condition.
Does sitting all day hurt my heart if I exercise later?
Yes. Prolonged sitting (sedentary behaviour) is an independent risk factor. Even if you go to the gym, sitting for 8+ hours slows down metabolism. Regular ‘movement breaks’ are essential.
Can losing weight reverse coronary artery disease?
Weight loss can lower blood pressure, cholesterol, and blood sugar, which stops the progression of the disease and stabilises plaque, significantly reducing the risk of a heart attack.
Authority Snapshot
This article was written by Dr. Rebecca Fernandez, a UK-trained physician (MBBS) with extensive experience in internal medicine, cardiology, and preventive care. Drawing on her background in managing complex chronic conditions and supporting patient well-being, Dr. Fernandez explains the physiological impact of weight and activity on heart health. This content has been reviewed to ensure strict alignment with NHS and NICE safety guidelines, offering a clear, non-judgmental explanation of these critical risk factors.
