When is bypass surgery recommended for angina?
Angina is chest pain caused by reduced blood flow to the heart muscle, and while many cases are managed with medication or stents, bypass surgery remains a critical intervention for more severe cases. In the UK, Coronary Artery Bypass Grafting (CABG) is recommended when the heart’s arterial network is extensively damaged or when other treatments are unlikely to provide long term relief.
In this article, you will learn about the clinical criteria that lead to a surgical recommendation, including the complexity of the blockages and the presence of underlying conditions like diabetes. We will also explore the causes of severe angina, the triggers for surgical referral, and how bypass surgery differs from stenting in its long term achievements.
What We’ll Discuss in This Article
- Clinical indications for bypass surgery in stable and unstable angina
- Why multi vessel disease and Left Main Stem blockages require surgery
- The role of bypass surgery in patients with diabetes and reduced heart function
- How atherosclerosis causes the severe narrowings that lead to surgery
- Triggers that necessitate a transition from medication to surgical intervention
- Differentiating the outcomes of bypass surgery versus coronary stenting
- Emergency guidance for severe or worsening angina symptoms
Clinical indications for bypass surgery in angina patients
Bypass surgery is typically recommended for angina when a patient has ‘complex’ coronary artery disease that cannot be safely or effectively treated with stents. The most common indication is ‘triple vessel disease,’ where all three main coronary arteries are significantly narrowed. In these cases, surgery provides a more comprehensive restoration of blood flow than multiple stents.
Another critical indication is narrowing of the ‘Left Main Stem’ artery. Because this single vessel supplies the majority of the blood to the left side of the heart, any significant blockage here is considered high risk. UK clinicians frequently recommend bypass surgery for these patients because the surgical grafts provide a more durable and reliable ‘detour’ for blood flow than a stent in this high pressure location.
- Multi Vessel Disease: Significant narrowings in two or more major heart arteries.
- Left Main Stem Disease: A blockage in the primary ‘trunk’ artery of the heart.
- Complex Anatomy: Blockages at branching points or in heavily calcified vessels.
- Failed Prior Treatments: When angina symptoms persist despite optimal medication or previous stenting.
Why patient health profiles influence the decision
The recommendation for bypass surgery for angina is not based solely on X-ray images of the heart; it also depends on the patient’s overall health. One of the strongest clinical drivers for surgery over stenting is the presence of diabetes. Research has consistently shown that for diabetic patients with extensive coronary disease, bypass surgery offers a lower risk of future heart attacks and better long term survival.
Additionally, if the heart muscle has already started to weaken (reduced ejection fraction), a bypass is often preferred. By providing a new, high volume blood supply through multiple grafts, surgery can help preserve remaining heart function and prevent the progression of heart failure. A multidisciplinary ‘Heart Team’ of surgeons and cardiologists reviews these factors to ensure the safest pathway is chosen.
Causes of severe angina necessitating surgery
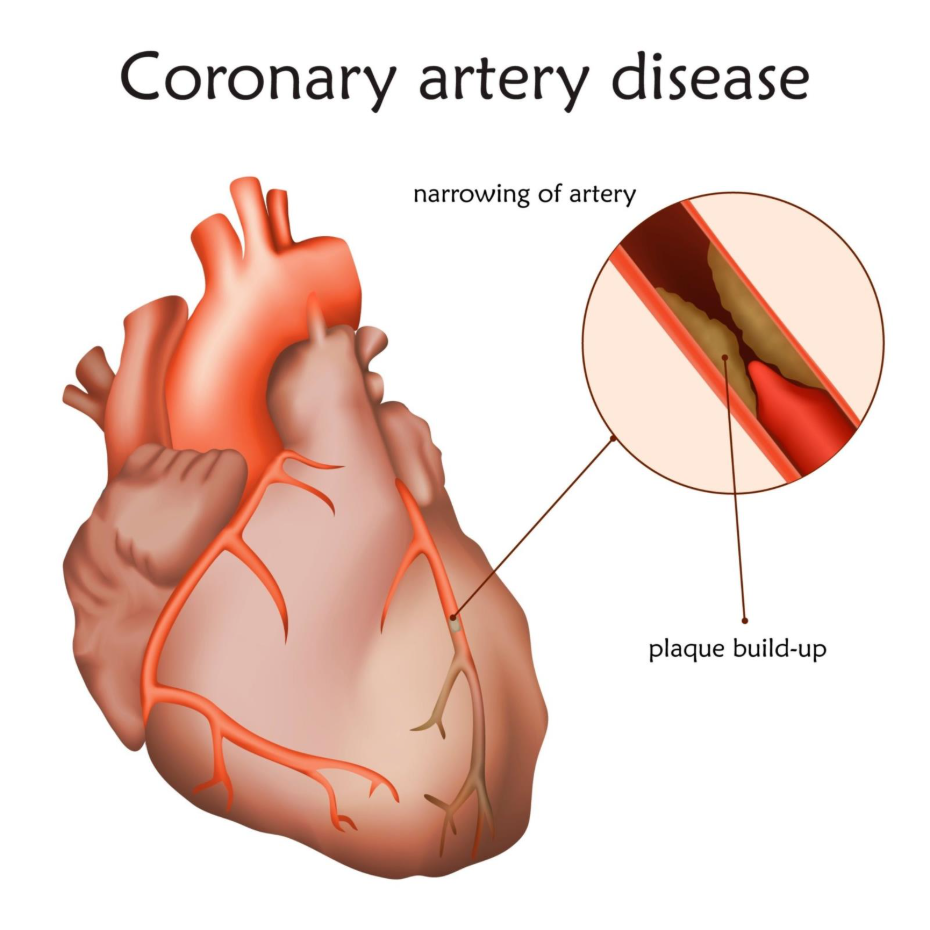
The primary cause of the severe arterial narrowings that lead to bypass surgery is atherosclerosis. This is a long term process where cholesterol, calcium, and fatty substances build up to form hard plaques in the artery walls. Over decades, these plaques grow, eventually reaching a point where they obstruct the majority of the vessel’s diameter (the lumen).
In patients referred for surgery, this atherosclerosis is often ‘diffuse,’ meaning it affects long stretches of the artery rather than one small spot. While a stent is designed to treat a ‘focal’ or short blockage, surgery is far better suited for diffuse disease because the graft simply jumps over the entire diseased section, landing on a healthier part of the artery further down.
- Chronic Inflammation: Long term damage to the artery lining from smoking or high blood pressure.
- Lipid Accumulation: High levels of LDL cholesterol contributing to plaque mass.
- Calcification: The hardening of plaques over time, making them difficult to stretch with a balloon.
- Microvascular Disease: In some cases, small vessel issues also contribute to the severity of the angina.
Triggers for surgical referral
Most patients with angina are managed with medications like beta blockers and nitrates for years. However, certain triggers can signal that it is time for a surgical referral. A ‘crescendo’ pattern of pain, where angina episodes become more frequent, occur with less effort, or start happening at rest (unstable angina), is a major trigger for urgent investigation.
Another trigger is the discovery of a ‘silent’ but high risk blockage during routine testing. If a stress test or a CT coronary angiogram shows that the heart is severely deprived of oxygen even if the patient feels relatively okay, a surgeon may recommend bypass to prevent a catastrophic heart attack in the future.
- Worsening Symptoms: Pain that is harder to control with standard medication.
- Low Exercise Tolerance: Angina triggered by very minimal walking or household tasks.
- Abnormal Stress Tests: Evidence of significant heart strain during diagnostic evaluations.
- Ischaemic Events: A minor heart attack that reveals more extensive underlying disease.
Differentiation: Bypass surgery vs. Stenting for angina
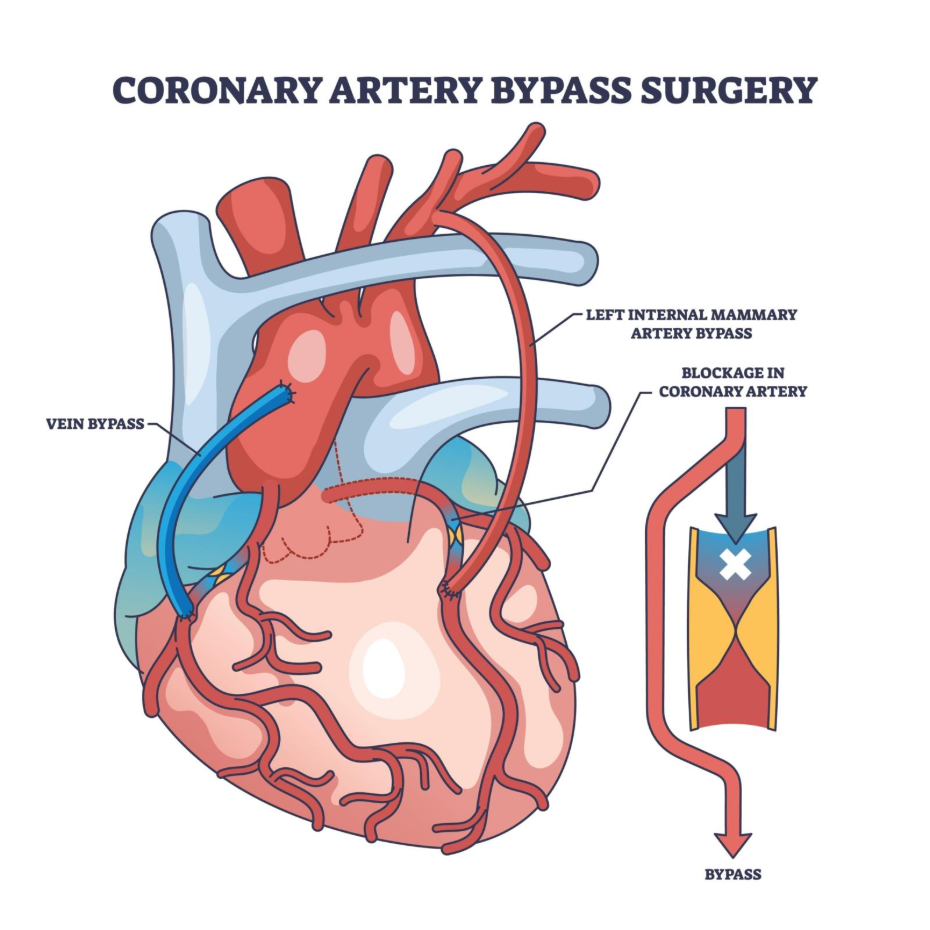
The fundamental difference between these two treatments lies in their approach to the blockage. A stent (PCI) is an ‘internal’ fix; it pushes the blockage out of the way to restore the original channel. Bypass surgery (CABG) is an ‘external’ fix; it ignores the blockage entirely and builds a new road around it using a vein from the leg or an artery from the chest.
While stenting is far less invasive and offers a recovery period of just a few days, bypass surgery is more durable for complex cases. Grafts used in surgery, particularly the internal mammary artery, have a very high likelihood of staying open for 15 to 20 years, whereas stents in complex areas have a slightly higher risk of narrowing again over time.
Conclusion
Bypass surgery is recommended for angina when the blockages are too complex for stents, especially in cases of multi vessel disease or Left Main Stem narrowing. It is the preferred option for patients with diabetes or reduced heart function, offering superior long term protection and symptom relief. While the recovery from surgery is longer, the achievement of complete revascularisation often leads to a better quality of life for those with severe heart disease.
If you experience severe, sudden, or worsening symptoms, such as crushing chest pain, fainting, or extreme shortness of breath, call 999 immediately.
Will bypass surgery cure my angina?
Bypass surgery is highly effective at relieving angina pain, but you must still manage the underlying heart disease with medication to prevent new blockages in the grafts.
How long is the wait for bypass surgery in the UK?
Waiting times vary by region and urgency; emergency cases are treated immediately, while elective cases are prioritised based on symptom severity.
Is bypass surgery considered safe?
Yes, it is a very well established procedure with high success rates in the UK, though like all major surgeries, it carries specific risks that your surgeon will discuss.
Will I still need to take tablets after the operation?
Yes, you will likely continue taking aspirin, statins, and possibly blood pressure medication to protect your new bypass grafts.
How long is the recovery period?
Most patients stay in the hospital for 5 to 7 days and require 6 to 12 weeks at home before returning to full activity.
Can I have stents instead if I am afraid of surgery?
In some cases, yes, but if your Heart Team recommends surgery, it is usually because stents are either too risky or unlikely to work in the long term for your specific blockages.
Can I have a bypass if I have already had a stent?
Yes, many people who have had stents in the past eventually require bypass surgery if their heart disease progresses or if the stents become blocked.
Authority Snapshot
This article was written by Dr. Rebecca Fernandez, a UK trained physician with an MBBS and extensive experience in cardiology, general surgery, and emergency medicine. Having managed critically ill patients and worked across diverse surgical settings in the NHS, Dr. Fernandez provides expert, evidence based insights into the management of complex coronary disease. This content adheres to NHS and NICE safety frameworks to ensure accurate and trustworthy health information.
