Can anatomical problems contribute to sleep apnoea?
Anatomical problems are a significant factor in the development of obstructive sleep apnoea because the physical structure of the head, neck, and throat determines the stability of the airway during sleep. While lifestyle factors like weight are frequently discussed, many individuals have an inherent physical predisposition that makes their airway more likely to collapse when muscles relax at night. Identifying these anatomical traits is a vital part of a clinical assessment and helps healthcare providers determine if surgical or mechanical interventions are necessary to maintain clear breathing.
What We’ll Discuss in This Article
- The impact of jaw and facial structure on airway stability
- How enlarged tonsils and adenoids restrict airflow during sleep
- The role of a naturally narrow throat or large tongue in obstruction
- Nasal issues and their contribution to sleep disordered breathing
- A comparison of soft tissue versus skeletal anatomical factors
- Clinical treatment options for correcting anatomical obstructions
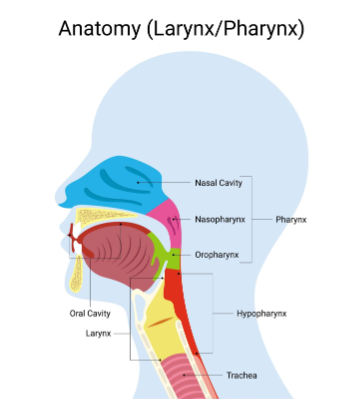
Anatomical problems contribute to sleep apnoea by physically reducing the space available for air to pass through the throat or by creating a structure that is easily blocked. Obstructive sleep apnoea (OSA) is caused by the walls of the throat relaxing and narrowing during sleep, which interrupts normal breathing. When the physical architecture of the airway is naturally small, even minor muscle relaxation can lead to a complete blockage, triggering the repeated waking and oxygen drops characteristic of the condition.
Jaw Structure and Craniofacial Morphology
The position and size of the jaw are primary skeletal factors that can determine the likelihood of experiencing sleep apnoea. In some individuals, the lower jaw is set further back than normal (retrognathia) or is unusually small (micrognathia), which reduces the space behind the tongue. When these individuals lie down to sleep, the tongue is more likely to fall backward against the soft palate and the back of the throat, causing an obstruction.
NICE clinical knowledge summaries note that anatomical risk factors for OSA include craniofacial abnormalities such as a recessed mandible or a narrow maxillary arch. These skeletal traits are often hereditary, explaining why sleep apnoea can sometimes run in families. Because the problem is structural, these patients may experience severe apnoea even if they maintain a healthy body weight, as the issue is related to bone placement rather than excess soft tissue.
Soft Tissue Obstructions
Beyond bone structure, the size and shape of the soft tissues within the throat play a critical role in airway clearance. Enlarged tonsils or adenoids are among the most common anatomical causes of sleep apnoea, particularly in children and some adults. These tissues can physically crowd the upper airway, making it difficult for air to flow freely. In many paediatric cases, the surgical removal of these tissues is the primary curative treatment for disordered breathing.
A large tongue (macroglossia) or a long, thick, soft palate can also contribute to the problem. These tissues take up valuable space in the narrowest part of the throat. During deep sleep, when muscle tone is at its lowest, these tissues can act like a physical plug. Individuals with these traits often find that their symptoms are significantly worse when sleeping on their back, as gravity pulls the heavy soft tissues directly into the breathing path.
Nasal Issues and Airway Vacuum
While obstructive sleep apnoea occurs in the throat, problems within the nose can significantly worsen the condition by forcing mouth breathing and increasing airway “suction.” A deviated septum, nasal polyps, or chronic inflammation can restrict nasal airflow. When the nose is blocked, the body must work harder to pull air through the throat, creating a vacuum effect that makes the walls of the throat more likely to collapse inward.
| Anatomical Feature | Impact on the Airway |
| Small Lower Jaw | Pushes the tongue backward into the breathing space. |
| Enlarged Tonsils | Physically narrows the width of the throat passage. |
| Thick Neck | Increases external pressure on the airway walls. |
| Nasal Deviation | Forces mouth breathing and increases throat suction. |
Addressing these nasal issues alone may not cure sleep apnoea if the primary blockage is in the throat, but it often improves the effectiveness of other treatments. For example, clearing nasal passages can make it easier for a patient to tolerate Continuous Positive Airway Pressure (CPAP) therapy, as they can breathe more comfortably through their nose while wearing the mask.
Conclusion
Anatomical problems such as a small jaw, enlarged tonsils, or a narrow throat are major contributors to sleep apnoea because they physically compromise the airway. These structural factors often interact with muscle relaxation during sleep to cause repeated breathing interruptions. Identifying these physical traits through a clinical examination is essential for tailoring an effective treatment plan, which may include dental devices or surgery. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can I have sleep apnoea if I am thin?
Yes, if you have anatomical issues like a narrow throat or a recessed jaw, you can develop sleep apnoea regardless of your weight.
Are tonsils always removed for sleep apnoea?
Tonsillectomy is a common treatment for children with sleep apnoea but is only recommended for adults if the tonsils are significantly enlarged and causing obstruction.
Does a deviated septum cause sleep apnoea?
A deviated septum does not directly cause apnoea in the throat, but it can worsen the condition by making it harder to breathe through the nose.
Can jaw surgery cure sleep apnoea?
In some severe cases where the jaw is the primary cause, surgical repositioning of the jaw can be an effective way to permanently open the airway.
Is the shape of my throat hereditary?
Yes, craniofacial structures like jaw size and throat width are often inherited, which is why sleep apnoea can run in families.
What is a “long uvula” and does it matter?
A long uvula (the tissue hanging at the back of the throat) can vibrate more easily, contributing to loud snoring and potentially blocking the airway.
How do doctors check for anatomical problems?
Clinicians may use a physical examination of the mouth and neck, or in some cases, imaging like X-rays or endoscopy, to assess your airway structure.
Authority Snapshot (E-E-A-T Block)
This article examines the anatomical and structural causes of sleep apnoea to provide the public with safe, evidence-based health information. It was written by the MyPatientAdvice Medical Content Team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine and emergency care. All information presented is strictly aligned with current NHS and NICE clinical guidance to ensure medical accuracy.
