Is joint hypermobility linked to OA?
The relationship between joint hypermobility and osteoarthritis is a complex area of clinical interest, as the very flexibility that allows for an extended range of motion can sometimes increase the long-term risk of joint changes. Hypermobility, often described as being ‘double-jointed’, occurs when the ligaments and connective tissues that hold a joint in place are more elastic than usual. While this trait can be an advantage in certain activities, it can also lead to a persistent state of subtle joint instability. When a joint is ‘loose’, the bones may not glide and roll in a perfectly aligned path, leading to uneven mechanical stress and increased friction on the articular cartilage. Over many decades, this ‘abnormal loading’ can overwhelm the body’s natural repair mechanisms, potentially accelerating the thinning of the protective cartilage. Understanding this link is essential for those with hypermobile joints, as it shifts the focus toward building ‘active’ stability through muscle strengthening. By protecting these more flexible joints from excessive wear, individuals can enjoy their natural mobility while significantly reducing the likelihood of developing osteoarthritis in later life.
What We’ll Discuss in This Article
- The clinical link between joint laxity and osteoarthritis risk
- How hypermobility causes uneven mechanical stress on cartilage
- The biological impact of chronic joint instability and micro-trauma
- Why certain joints like the knees, hips, and thumbs, most affected
- The role of proprioception and muscle strength in protecting flexible joints
- Identifying common triggers that increase the risk of wear in hypermobile joints
- The importance of differentiating hypermobility from other connective tissue conditions
Understanding joint laxity and mechanical stress
Joint hypermobility is characterised by an increased range of motion beyond what is considered normal for a specific joint. This is usually due to the structure of the collagen within the ligaments, which is more stretchy than average. While this is not a disease in itself, it does change the mechanics of how the joint handles weight and movement.
In a standard joint, the ligaments act as strong ‘passive’ stabilisers that keep the bones perfectly aligned during movement. In a hypermobile joint, these stabilisers are less effective, allowing the joint surfaces to shift or ‘shear’ against each other. The NHS notes that this shifting creates concentrated pressure points on the cartilage. Much like a tyre that is slightly out of alignment on a car, a hypermobile joint may experience faster, uneven wear on certain patches of cartilage, which is a primary driver of the structural changes seen in osteoarthritis.
Chronic instability and the ‘Wear and Repair’ cycle
The joints are living systems that constantly perform a ‘wear and repair’ cycle. In hypermobility, the joint is frequently subjected to ‘micro-trauma’, tiny, often painless disruptions to the cartilage and joint lining caused by abnormal movement. While the body attempts to repair these areas, the persistent instability can eventually outpace the repair process.
Clinical evidence suggests that this chronic instability can trigger low-grade inflammation within the joint lining (synovium). As the body tries to stabilise a joint it perceives as ‘loose’, it may produce bony spurs (osteophytes) at the edges of the joint. In hypermobile individuals, these spurs are a sign that the body is attempting to widen the joint surface to create more stability, even though the underlying issue is the elasticity of the soft tissues. Supporting the joint through targeted strengthening helps to provide the stability that the ligaments cannot, protecting the cartilage from this cycle of disorganised repair.
Joints most vulnerable to hypermobility-related OA
Hypermobility does not affect all joints equally, and certain areas of the body are more prone to developing osteoarthritis as a result of excessive flexibility.
- The Knees: Hypermobile knees often hyperextend (bend backward), which puts immense pressure on the front of the joint and the cartilage behind the kneecap.
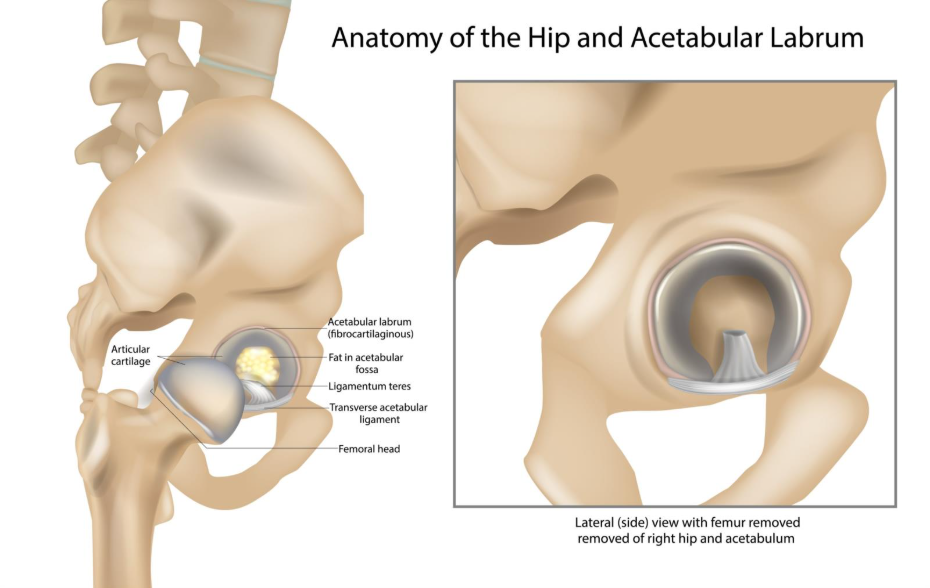
- The Hips: Excessive range of motion in the hip can lead to labral tears and faster thinning of the cartilage in the socket.
- The Thumbs: The base of the thumb is frequently hypermobile, and the constant ‘subluxing’ (partial slipping) of this joint during daily tasks is a leading cause of early hand osteoarthritis.
- The Spine: Increased flexibility in the small joints of the back can lead to postural issues and uneven loading of the vertebrae.
Recognising which of your joints are most flexible allows you to focus your strengthening efforts on the specific muscles that provide stability to those vulnerable areas.
The role of proprioception and muscle control
Individuals with hypermobile joints often have reduced proprioception, the body’s ability to sense exactly where a joint is in space. Because the ligaments are stretchy, they send less ‘tension’ data to the brain, which can lead to awkward movements or overextending the joint without realising it. This lack of sensory feedback increases the risk of micro-injuries that contribute to osteoarthritis.
Clinical guidance from NICE emphasises that the most effective way to protect hypermobile joints is through ‘proprioceptive training’ and muscle strengthening. Muscles act as ‘active’ stabilisers. When the muscles around a flexible joint are strong and well-coordinated, they take the strain off the ligaments and ensure the joint stays within its safe, healthy range of motion. This ‘muscular sleeve’ is the best protection against the long-term wear that leads to osteoarthritis.
Investigating the causes of hypermobile flares
For those with hypermobility, the joints can be more sensitive to daily stresses, leading to frequent ‘flares’ of aching and stiffness. These episodes are often the result of the soft tissues and joint lining becoming irritated by excessive movement.
Typical triggers for hypermobile joint pain include:
- Prolonged Standing: Gravity can cause hypermobile joints to ‘settle’ into their end-range of motion, putting static stress on the cartilage.
- High-Impact Exercise: Activities like running or jumping can be difficult for joints that lack firm passive stability.
- Fatigue: When the muscles get tired, they can no longer protect the flexible joint, leading to immediate mechanical stress on the cartilage.
- Hormonal Changes: For women, fluctuations in hormones like progesterone can make ligaments even more elastic at certain times of the month, increasing joint instability.
Identifying triggers for symptom flare-ups
Recognising the early warning signs of joint irritation, such as a deep ache or a feeling that the joint is ‘loose’, can help you intervene before the symptoms become severe. This might involve wearing a temporary support, switching to lower-impact movements like swimming, or focusing on gentle isometric exercises that engage the muscles without moving the joint through its full range. By managing these triggers proactively, you can support your joint’s natural repair mechanisms and maintain your flexibility without sacrificing your long-term joint health.
Differentiation: Hypermobility vs Inflammatory Conditions
It is important to differentiate between the joint pain of hypermobility and that caused by inflammatory conditions like rheumatoid arthritis or lupus. While hypermobility causes pain related to movement and instability, inflammatory arthritis is an autoimmune condition where the immune system attacks the joint lining. Inflammatory conditions often cause significant swelling, heat, and morning stiffness that lasts for hours, whereas hypermobility-related pain is usually mechanical and worsens after activity. If your flexible joints are accompanied by extreme fatigue, widespread skin rashes, or if your joints become very red and hot, you should seek a medical evaluation to rule out a systemic connective tissue or autoimmune issue.
Conclusion
Joint hypermobility is linked to osteoarthritis primarily through the increased mechanical stress and instability that ‘loose’ joints place on the articular cartilage. While being flexible is a natural trait, it requires a proactive approach to joint care to ensure the cartilage is not subjected to uneven wear over time. By building strong supporting muscles and improving proprioception, individuals can effectively provide the stability their ligaments lack, protecting the joints from the structural changes of osteoarthritis. Most people with hypermobility find that with the right strengthening routine and awareness of their joint alignment, they can maintain a highly active lifestyle while preserving their long-term joint health.
If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is hypermobility a type of arthritis?
No. Hypermobility is a trait of the connective tissues, but it can be a risk factor for developing osteoarthritis later in life due to joint instability.
Can I be hypermobile and still have stiff joints?
Yes. Sometimes the muscles around a hypermobile joint become chronically tight as they try to ‘work overtime’ to provide the stability the ligaments are not providing.
Should I stop stretching if I am hypermobile?
It is generally better to focus on strengthening and stability rather than further stretching of the ligaments, although gentle muscle stretching is usually fine.
Why does my thumb click so much?
In hypermobile individuals, the base of the thumb often partially slips out of its socket (subluxation) during use, which is a common cause of clicking and early osteoarthritis.
Can children with hypermobility get OA?
Osteoarthritis is rare in children, but the joint instability seen in hypermobile children can set the stage for joint changes to occur earlier in adulthood.
Does weight loss help with hypermobile joint pain?
Yes. Reducing body weight significantly lowers the mechanical load that your flexible joints and supporting muscles have to manage.
Authority Snapshot
This article was written by Dr. Stefan Petrov, a UK-trained physician with an MBBS and postgraduate certifications including Basic Life Support (BLS), Advanced Cardiac Life Support (ACLS), and the UK Medical Licensing Assessment (PLAB 1 & 2). He has hands-on experience in general medicine, surgery, anaesthesia, ophthalmology, and emergency care. Dr. Petrov has worked in both hospital wards and intensive care units, performing diagnostic and therapeutic procedures, and has contributed to medical education by creating patient-focused health content and teaching clinical skills to junior doctors.
