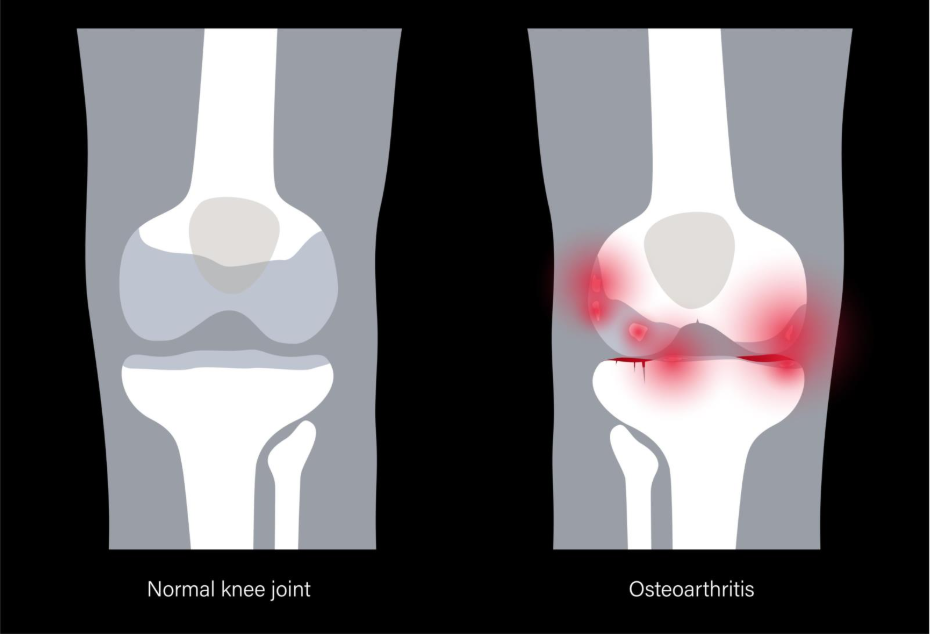
What will an X-ray show in OA?
While a clinical diagnosis of osteoarthritis is often made through a physical examination and a review of symptoms, an X-ray provides a valuable look at the structural changes occurring within the joint. Because X-rays primarily capture dense materials like bone, they do not show the articular cartilage itself; however, they reveal the ‘footprints’ of the condition through the way the bones react to its thinning. In a healthy joint, an X-ray shows a clear, even gap between the bone ends, representing the space occupied by healthy cartilage. In a joint affected by osteoarthritis, this gap may narrow, and the underlying bone may develop distinct features as it attempts to adapt to increased mechanical pressure. Understanding what an X-ray shows, from the growth of bony spurs to the thickening of the bone surface, helps to bridge the gap between the internal physical changes and the sensations of pain and stiffness you may experience. By identifying these characteristic signs, healthcare professionals can assess the extent of the structural changes and ensure that your management plan is tailored to your specific joint health needs.
What We’ll Discuss in This Article
- The primary structural signs of osteoarthritis on an X-ray
- Understanding joint space narrowing and its clinical significance
- The formation of osteophytes and why the body grows new bone
- Subchondral sclerosis and the thickening of the bone surface
- The appearance of subchondral cysts in more advanced stages
- Why X-ray findings do not always correlate with pain severity
- The importance of differentiating these signs from other bone conditions
Joint space narrowing
One of the most characteristic signs of osteoarthritis on an X-ray is joint space narrowing. In a healthy joint, the two bones do not actually touch; they are separated by a layer of articular cartilage. Since cartilage is a soft tissue that X-rays pass through, it appears as a dark, empty-looking ‘space’ on the image.
When the cartilage thins due to osteoarthritis, the bones move closer together, and this gap becomes visibly smaller. This narrowing is often asymmetrical, meaning it might be more pronounced on one side of the joint than the other. For example, in knee osteoarthritis, the narrowing is frequently seen on the inner (medial) side of the joint. This finding is a key indicator for clinicians that the protective cushioning is being lost, even though the cartilage itself cannot be seen directly.
Osteophytes: The growth of bony spurs
As the joint attempts to repair itself and distribute weight over a larger area, it often produces new bone at the edges of the joint. These growths are known as osteophytes or bony spurs. On an X-ray, they appear as small, pointed, or rounded protrusions extending from the original bone line.
While these spurs are a hallmark of the ‘wear and repair’ cycle, they are a permanent structural change. They can sometimes be felt as hard lumps near the skin, such as the nodes commonly seen in the fingers. According to clinical standards followed by the NHS, the presence of osteophytes is one of the most reliable radiological signs used to confirm the presence of osteoarthritis. While they are the body’s attempt to stabilise the joint, they can occasionally interfere with smooth movement or irritate surrounding soft tissues.
Subchondral sclerosis: Thickening of the bone
When the protective cartilage thins, the bone directly underneath it, the subchondral bone, is subjected to much higher levels of mechanical stress. In response to this pressure, the bone becomes denser and thicker, a process known as subchondral sclerosis.
On an X-ray, this appears as areas of increased whiteness (brightness) at the ends of the bones where they meet. This ‘whitening’ indicates that the bone has become more compact to handle the load. While this makes the bone stronger in that specific area, it also makes it less flexible and less effective at absorbing shocks. This finding helps explain why an affected joint might feel less ‘springy’ and more prone to deep, aching pain during weight-bearing activities.
Subchondral cysts
In more advanced stages of osteoarthritis, an X-ray may show subchondral cysts. These are small, fluid-filled pockets that form just beneath the surface of the bone. On an X-ray, they appear as tiny, dark, circular ‘holes’ or translucent areas within the white, sclerotic bone.
These cysts form when the increased pressure within the joint forces synovial fluid through microscopic cracks in the bone surface. While the term ‘cyst’ can sound concerning, in this context, they are simply a common feature of the joint’s structural adaptation. Clinical guidance from NICE suggests that the presence of these cysts, alongside narrowing and spurs, provides a comprehensive picture of a joint undergoing significant structural transition.
Investigating the ‘Scan vs. Symptom’ Gap
A vital aspect of understanding X-ray results is recognising that the severity of the changes seen on the image does not always match the severity of the pain a person feels. This is a common clinical observation known as the ‘discordance’ between imaging and symptoms.
Some people may have X-rays that show ‘severe’ osteoarthritis, with significant narrowing and many spurs, yet they experience very little pain and maintain excellent mobility. Conversely, others may have ‘mild’ changes on their scan but suffer from significant discomfort and stiffness. This happens because pain is influenced by many factors that an X-ray cannot see, such as the level of inflammation in the joint lining, the strength of the supporting muscles, and the sensitivity of the nervous system. This is why doctors treat the person, not just the X-ray.
Identifying triggers for a diagnostic scan
While many diagnoses are made without imaging, certain triggers may lead a healthcare professional to request an X-ray. If your symptoms are particularly severe, if the joint feels unstable or ‘locks’, or if you have had a previous injury in that area, a scan can help clarify the current structural state of the joint. It is also a necessary step if surgery, such as a joint replacement, is being considered. By identifying the specific location of the narrowing and the size of any osteophytes, a surgeon can plan the most effective approach to restoring your mobility.
Differentiation: OA signs vs Other bone conditions
It is important to differentiate the signs of osteoarthritis on an X-ray from other conditions. For example, rheumatoid arthritis often shows ‘erosions’, areas where the bone has been eaten away by inflammation, rather than the bony growths (osteophytes) seen in osteoarthritis. Conditions like osteoporosis involve a general thinning of the bone throughout the body, whereas the changes in osteoarthritis are localised to the affected joint. Furthermore, sudden changes or ‘ragged’ bone edges might suggest an infection or other rare bone issues. A healthcare professional will look for the specific ‘triad’ of narrowing, sclerosis, and osteophytes to confirm that the changes are indeed the result of the ‘wear and repair’ process of osteoarthritis.13
Conclusion
An X-ray of a joint affected by osteoarthritis typically shows a combination of joint space narrowing, the formation of bony spurs (osteophytes), and a thickening of the bone surface (sclerosis). These signs represent the body’s active attempt to adapt to the thinning of articular cartilage and the resulting increase in mechanical pressure.15 While these structural changes are permanent, they are only one part of the story. Because X-ray findings do not always correlate with the level of pain experienced, they are used alongside a physical examination and symptom history to create a complete picture of your joint health. By understanding what these images reveal, you can better understand the physical reality of your condition and focus on management strategies, such as strengthening supporting muscles, that improve your function regardless of what is seen on the scan.
If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why doesn’t the X-ray show my cartilage?
Cartilage is a soft tissue that is not dense enough to block X-rays; it appears as the ’empty’ space between the bones on the final image.
Does a ‘bone spur’ mean I need surgery?
No. Most bone spurs do not require surgery and are simply a common sign that the joint has adapted to changes in pressure.
Why is my joint space only narrow on one side?
Osteoarthritis often affects joints unevenly, with the side that carries the most mechanical load thinning faster than the other.
Can an X-ray show if my arthritis is ‘new’ or ‘old’?
While it can’t give an exact date, the presence of large osteophytes and subchondral cysts usually suggests that the changes have been occurring over a long period.
Is it possible to have OA if my X-ray is normal?
Yes. In the very early stages, the cartilage may have started to thin, but not enough to significantly narrow the joint space visible on an X-ray.
Does the X-ray show the fluid in my joint?
A standard X-ray does not clearly show fluid, but a large ‘effusion’ may sometimes be suspected if the bones appear slightly further apart or if the soft tissue shadows look enlarged.
Authority Snapshot
This article was written by Dr. Stefan Petrov, a UK-trained physician with an MBBS and postgraduate certifications including Basic Life Support (BLS), Advanced Cardiac Life Support (ACLS), and the UK Medical Licensing Assessment (PLAB 1 & 2). He has hands-on experience in general medicine, surgery, anaesthesia, ophthalmology, and emergency care. Dr. Petrov has worked in both hospital wards and intensive care units, performing diagnostic and therapeutic procedures, and has contributed to medical education by creating patient-focused health content and teaching clinical skills to junior doctors.
