What brain changes cause frontotemporal dementia?
Frontotemporal dementia is a distinct group of neurodegenerative disorders acterised by the progressive loss of neurons in the frontal and temporal lobes of the brain. In a clinical context, these brain regions are responsible for executive function, social behaviour, personality, and language. Unlike Alzheimer disease, which often begins in the memory centres, frontotemporal dementia targets the areas that define our social identity and communication skills.
The underlying brain changes involve a complex interplay of protein misfolding, genetic mutations, and cellular starvation. As specific proteins clump together inside brain cells, they disrupt vital internal processes, eventually leading to cell death and a visible shrinking of the brain tissue. This guide explores the biological mechanisms behind these changes and how they result in the unique clinical symptoms of the condition.
what we will discuss in this article
- The role of tau and TDP 43 protein accumulation
- Understanding focal atrophy in the frontal and temporal lobes
- The impact of genetic mutations like C9orf72 and MAPT
- How protein clumps disrupt cellular transport and energy
- The breakdown of neurotransmitter pathways in social regions
- The link between frontotemporal dementia and motor neurone disease
- emergency guidance for identifying signs of health deterioration
Protein aggregation: Tau and TDP 43
The primary driver of cell damage in frontotemporal dementia is the abnormal clumping of proteins inside the neurons.
Tau protein pathology
In about half of all cases, the damage is caused by the tau protein. Normally, tau acts as a stabiliser for microtubules, which are the internal tracks that transport nutrients within a cell. In frontotemporal dementia, tau misfolds and forms clumps called Pick bodies. These clumps destroy the neuron’s internal structure, leading to the behavioural and personality shifts seen in the clinic.
TDP 43 and FUS proteins
The other half of cases are primarily linked to a protein called TDP 43. This protein normally lives in the cell nucleus and helps regulate genetic instructions. When it malfunctions, it moves into the main body of the cell and forms toxic aggregates. A smaller number of cases involve the FUS protein. Regardless of the specific protein, the end result is the same: the neuron can no longer function and eventually dies.
Focal atrophy and structural changes
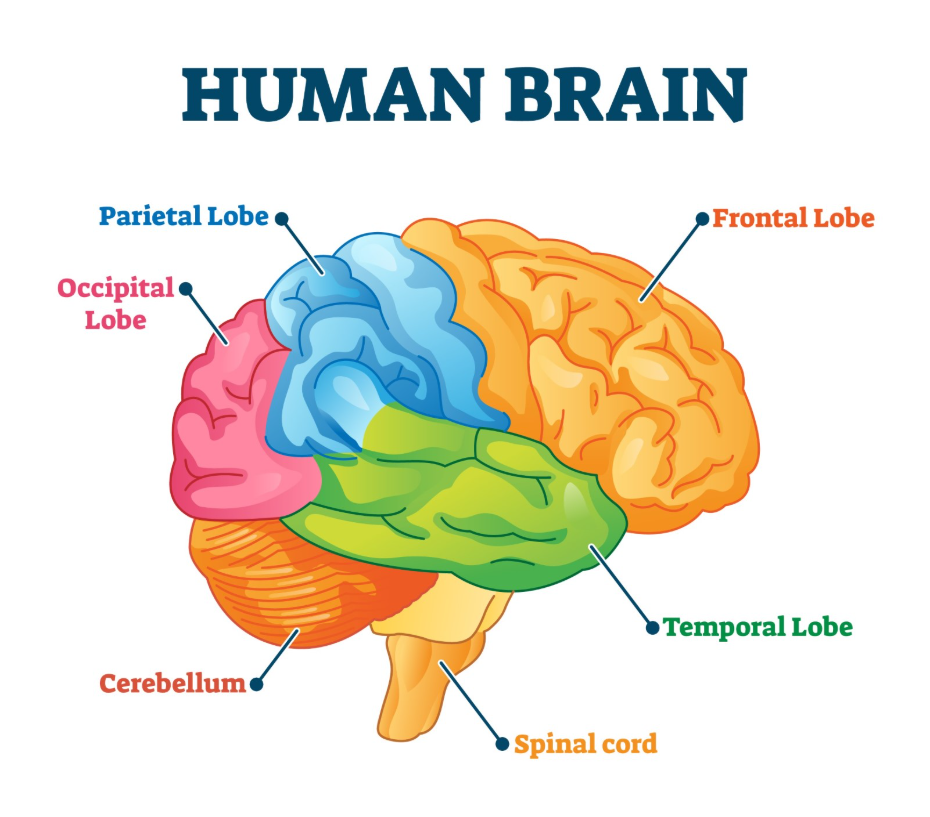
As neurons die off in large numbers, the brain begins to physically shrink in a process known as focal atrophy.
In frontotemporal dementia, this shrinkage is concentrated in the frontal lobes, located behind the forehead, and the temporal lobes, located behind the ears. On an MRI scan, clinicians can often see a stark contrast between these shrunken regions and the relatively healthy looking posterior parts of the brain. This specific pattern of atrophy explains why a person might lose their social filter or ability to speak while their visual memory and spatial orientation remain remarkably intact for many years.
The role of genetics
Frontotemporal dementia has a stronger genetic component than many other forms of neurodegeneration. Approximately one third of cases are hereditary. Three specific genes are most commonly involved:
- C9orf72: This is the most common genetic cause and is unique because it can cause both frontotemporal dementia and motor neurone disease, sometimes within the same family.
- MAPT: This gene provides the instructions for making tau protein. Mutations here lead directly to the formation of toxic tau clumps.
- GRN: This gene helps produce progranulin, a protein that supports cell survival and regulates inflammation.
Comparison of pathological markers
| Feature | Tau Positive FTD | TDP 43 Positive FTD |
| Primary Protein | Tau (Pick bodies) | TDP 43 |
| Common Subtype | Behavioural variant | Semantic variant / FTD with MND |
| Genetic Link | Often MAPT mutations | Often C9orf72 or GRN mutations |
| Cellular Location | Inside the main cell body | Moves from nucleus to cytoplasm |
Neurotransmitter disruption
Beyond physical cell loss, the brain changes also involve a failure of chemical signalling. The damage specifically targets pathways that use serotonin and dopamine, which are essential for regulating mood, impulse control, and motivation.
This chemical imbalance is what leads to the profound apathy or the impulsive, socially inappropriate behaviours characteristic of the behavioural variant. Unlike Alzheimer disease, the acetylcholine system, which is involved in memory, is often spared in the early stages, which is why memory medications frequently do not work for this condition.
To summarise
Frontotemporal dementia is caused by a devastating combination of protein toxicity, genetic vulnerability, and focal brain shrinkage. Whether driven by tau or TDP 43, the resulting death of neurons in the frontal and temporal lobes strips away a person’s social and linguistic abilities. Understanding these specific brain changes is vital for a correct clinical diagnosis and for developing targeted therapies. While the damage is currently irreversible, research into the genetic and molecular roots of the disease offers hope for future interventions that can protect these critical brain regions.
emergency guidance
Acute medical or behavioural crises in frontotemporal dementia require immediate action. Call 999 or seek urgent clinical help if a person becomes physically aggressive and poses a danger to themselves or others, or if they exhibit a sudden loss of consciousness. Because the condition can eventually affect movement and coordination, a sudden inability to swallow is a medical emergency that carries a high risk of choking or aspiration pneumonia. Any rapid and severe change in a person’s physical or cognitive state must be assessed by an emergency medical team to rule out acute issues like a stroke or infection.
Why does this dementia happen to younger people?
The reasons are not fully understood, but the strong genetic link in frontotemporal dementia may contribute to its earlier onset compared to Alzheimer disease.
Can a brain scan prove it is FTD?
An MRI can show the specific pattern of frontal and temporal shrinkage, which is a very strong indicator, though it must be combined with a clinical history.
Is there a test for the TDP 43 protein?
While researchers can identify these proteins in brain tissue after death, there is currently no standard clinical test to see which protein is causing the damage in a living person.
What is the link to motor neurone disease?
The C9orf72 gene mutation can cause both conditions, leading to a specific subtype where the person experiences both personality changes and progressive muscle weakness.
Does the brain shrinkage happen quickly?
The speed of atrophy varies, but frontotemporal dementia often progresses more rapidly than some other forms of neurodegeneration.
Can we stop the protein clumping?
There are no approved treatments to stop protein aggregation yet, but many clinical trials are currently targeting the tau and progranulin pathways.
Authority Snapshot
Dr. Rebecca Fernandez is a UK trained physician with an MBBS and experience in general surgery, cardiology, internal medicine, gynecology, intensive care, and emergency medicine. She has managed critically ill patients, stabilised acute trauma cases, and provided comprehensive inpatient and outpatient care. In psychiatry, Dr. Fernandez has worked with psychotic, mood, anxiety, and substance use disorders, applying evidence based approaches such as CBT, ACT, and mindfulness based therapies. Her skills span patient assessment, treatment planning, and the integration of digital health solutions to support mental well being in 2026.
