

Frontotemporal dementia is a relatively rare but significant form of dementia that primarily affects the frontal and temporal lobes of the brain. In a clinical context, it is distinguished from other forms of dementia because it often occurs at a younger age, typically appearing in individuals between 45 and 65 years old. Because the frontal and temporal lobes are responsible for personality, social behaviour, and language, the initial symptoms often involve dramatic changes in character and communication skills rather than the memory loss associated with Alzheimer disease.
The condition is progressive and results from the physical degeneration of brain tissue in these specific regions. As the nerve cells die, the lobes begin to shrink: a process known as atrophy. This leads to a gradual loss of function that can be deeply distressing for both the individual and their family, as the person’s personality and social inhibitions may change entirely. Understanding the biological causes and the different variants of frontotemporal dementia is essential for providing appropriate clinical support and managing the unique behavioural challenges it presents.
What we will discuss in this article
- The clinical definition of frontotemporal dementia as a localized brain disorder
- The role of abnormal protein buildup in causing nerve cell death
- Identifying the primary behavioural and personality changes
- Understanding the language variants and their impact on communication
- The significant genetic link and family history in frontotemporal dementia
- How the condition differs from other types of dementia in younger patients
- Emergency guidance for identifying signs of health deterioration
The biological causes of frontotemporal dementia
Frontotemporal dementia is caused by the accumulation of abnormal proteins that are toxic to brain cells.
Protein clumping and atrophy
The primary cause of the damage is the clumping together of specific proteins inside the neurons of the frontal and temporal lobes. The most common proteins involved are tau and TDP 43. When these proteins misfold and aggregate, they disrupt the normal functioning of the cell, leading to its eventual death. As millions of cells die, the physical structure of the brain changes. On a clinical MRI scan, this is visible as significant thinning or shrinking of the frontal and temporal areas. Historically, this condition was sometimes referred to as Pick disease when specific protein clumps were present.
Variants and their impact on behaviour and language
The symptoms of frontotemporal dementia depend on which part of the brain is damaged first. This leads to several distinct clinical variants.
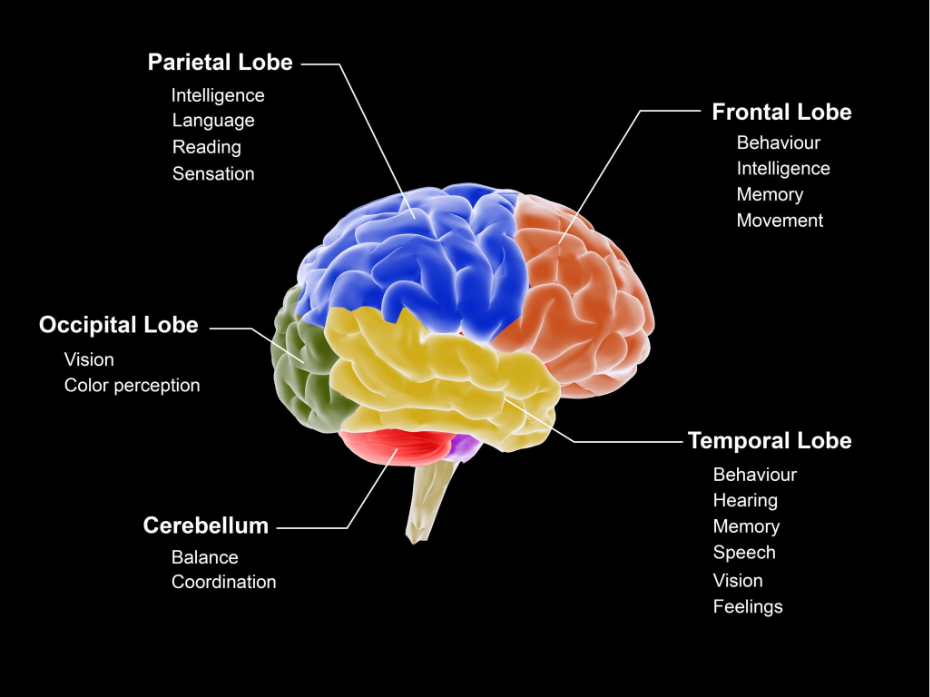
Behavioural variant
This is the most common form and primarily affects the frontal lobe. This region is responsible for executive functions, such as planning and decision making, as well as social conduct. Damage here leads to loss of inhibition, impulsivity, and a lack of empathy. A person might start acting inappropriately in social situations, become obsessive, or show a marked lack of interest in things they once cared about.
Primary progressive aphasia
This variant primarily targets the temporal lobes, which are the main centres for language and communication. It is further divided into subtypes: one where the person loses the ability to find words or understand their meaning, and another where the person has difficulty physically producing speech even though they know what they want to say. In these cases, cognitive functions like memory and orientation may remain intact for many years while communication declines.
Comparison of frontotemporal dementia variants
| Variant | Primary Brain Region | Key Symptoms |
| Behavioural Variant | Frontal Lobe | Impulsivity, loss of empathy, social changes |
| Semantic PPA | Temporal Lobe Left | Loss of word meanings and object names |
| Non fluent PPA | Frontal and Temporal Left | Slow, hesitant speech and grammar issues |
| FTD MND | Frontal Lobe and Motor Cortex | Behaviour changes plus muscle weakness |
| Corticobasal Syndrome | Multiple regions | Coordination issues and behavioural changes |
Genetics and family history
Frontotemporal dementia has a much stronger genetic component than most other forms of dementia.
Research indicates that approximately one-third to one-half of people with the condition have a family history of dementia or related neurological issues. In about 10 to 20 per cent of cases, a specific genetic mutation can be identified as the direct cause. The most common genes involved are C9orf72, MAPT, and GRN. Because of this strong link, clinical genetic counselling is often recommended for families where multiple members have been affected by frontotemporal dementia or motor neurone disease.
How it differs from other dementias
Frontotemporal dementia is often misdiagnosed as a psychiatric condition or Alzheimer disease because of its early onset and unusual symptoms.
Unlike Alzheimer, memory is often well preserved in the early and middle stages of frontotemporal dementia. The person may still remember the names of their children and find their way around the house, but their personality may have changed so much that they no longer seem like the same person. Furthermore, because it often affects people who are still in their working years, the impact on employment and family dynamics is unique, requiring a specialised clinical approach that addresses both the neurological and social challenges.
To summarise
Frontotemporal dementia is a localised neurodegenerative disease caused by the death of nerve cells in the frontal and temporal lobes. Driven by the toxic buildup of proteins like tau and TDP-43, the condition leads to progressive changes in personality, social behaviour, and language skills. With a significant genetic component and an earlier age of onset than Alzheimer, it requires careful clinical diagnosis and specialised support. While there is currently no cure, understanding the specific brain regions involved allows for better management of symptoms and more focused care for both the individual and their family.
Emergency guidance
While frontotemporal dementia progresses slowly, sudden changes in behaviour or safety require urgent clinical attention. Call 999 or seek immediate medical help if a person with the condition becomes a danger to themselves or others due to extreme impulsivity or aggression. You should also seek urgent care if they show signs of motor neurone disease, such as sudden difficulty swallowing or severe muscle weakness, as these conditions sometimes overlap. Rapid clinical assessment is necessary to manage acute behavioural crises and ensure the safety of the individual and their caregivers.
Is frontotemporal dementia the same as Pick disease?
Pick disease is a specific type of frontotemporal dementia characterised by the presence of Pick bodies, which are spherical clumps of tau protein. Today, frontotemporal dementia is used as the broader umbrella term.
How is frontotemporal dementia diagnosed?
Diagnosis involves a thorough clinical assessment, neuropsychological testing of behaviour and language, and brain imaging like MRI or PET scans to look for specific patterns of atrophy or reduced metabolic activity.
Can it be treated?
There is no cure or medication specifically for frontotemporal dementia. Clinical management focuses on speech therapy, behavioural strategies, and sometimes medications to help with impulsivity or mood changes.
Is it always inherited?
No. While it has a strong genetic link, many cases are sporadic, meaning they occur in people with no known family history of the condition.
What is the life expectancy?
This varies depending on the variant and the individual. On average, people live for about eight to ten years after the symptoms start, but this can be much shorter if the condition is linked with motor neurone disease.
Why does it affect younger people?
Researchers are still investigating why the frontal and temporal lobes are more susceptible in younger adults. It is likely a combination of specific genetic vulnerabilities and the unique biology of those brain regions.
Authority Snapshot
Dr. Rebecca Fernandez is a physician with an MBBS and experience in general surgery, cardiology, internal medicine, gynecology, intensive care, and emergency medicine. She has managed critically ill patients, stabilised acute trauma cases, and provided comprehensive inpatient and outpatient care. In psychiatry, Dr. Fernandez has worked with psychotic, mood, anxiety, and substance use disorders, applying evidence based approaches such as CBT, ACT, and mindfulness based therapies. Her skills span patient assessment, treatment planning, and the integration of digital health solutions to support mental well being in 2026.
