


A brain tumour can cause seizures by irritating the surrounding electrical pathways of the brain and disrupting the normal signals between nerve cells. Seizures are one of the most common symptoms of both primary and secondary brain tumours, occurring when the presence of a growth or the associated swelling triggers a sudden burst of uncontrolled electrical activity. In the United Kingdom, healthcare professionals treat a first-time seizure in an adult as a clinical priority that requires urgent investigation to identify any structural causes within the skull. While many conditions can cause seizures, the pattern and nature of the fit often provide important clues about the tumour’s location and its impact on the brain’s functional health. Understanding the link between brain growths and electrical disruptions is essential for patients and their families to navigate the management process. By following evidence-based protocols established by the NHS and NICE, medical teams aim to control seizure activity through medication or surgery while addressing the underlying tumour.
What We’ll Discuss in This Article
- The biological mechanism of tumour-induced electrical irritation.
- Distinguishing between focal and generalised seizures.
- How the location of a tumour determines the type of fit.
- The clinical significance of a first-time seizure in adults.
- Management options for controlling seizures in tumour patients.
- UK clinical pathways for urgent neurological assessment and care.
Biological Mechanism of Tumour-Induced Seizures
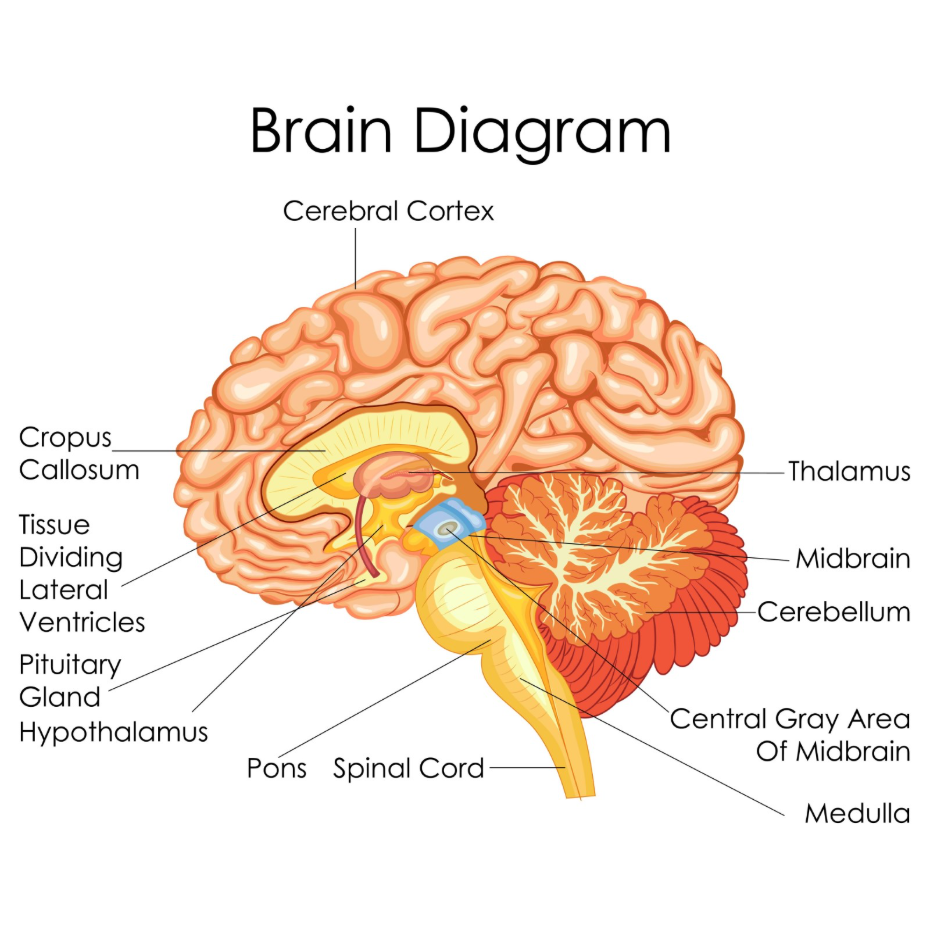
Seizures occur in patients with brain tumours because the abnormal mass disrupts the delicate chemical and electrical balance of the surrounding healthy brain tissue. The brain operates through a series of electrical impulses passed between neurons; when a tumour is present, it can compress these cells or cause “oedema,” which is a build-up of fluid that alters the local environment. The NHS states that a brain tumour can cause symptoms by increasing the pressure inside the skull or by damaging the part of the brain where the tumour is growing.
This irritation can make the neurons more likely to fire randomly or excessively, leading to a seizure. In some cases, the tumour itself may release certain chemicals that lower the threshold for electrical activity. In the United Kingdom, clinicians use this understanding to explain why even a small, slow-growing tumour can cause significant seizures if it is located in a highly sensitive area. The goal of management is to stabilise this electrical activity while addressing the physical growth.
Distinguishing Between Focal and Generalised Seizures
In the United Kingdom, seizures caused by brain tumours are broadly categorised into focal (partial) seizures or generalised seizures, depending on how much of the brain is involved in the electrical disruption. Focal seizures are the most common type seen in tumour patients and occur when the electrical burst is confined to a specific part of the brain. NICE clinical guidelines for brain tumours indicate that the nature of the seizure is a key diagnostic indicator that helps determine the likely location of the growth.
A focal seizure might manifest as a strange smell, a sudden wave of emotion, or twitching in a single limb, often without the person losing consciousness. Generalised seizures involve the entire brain and usually result in a loss of consciousness and rhythmic muscle jerking.
| Seizure Type | Clinical Presentation | Typical Involvement |
| Focal (Simple) | Twitching; sensory changes; remains awake. | Limited to one area of one hemisphere. |
| Focal (Complex) | Confusion; repetitive movements; altered awareness. | Spreads but remains localised. |
| Generalised | Loss of consciousness; stiffening; jerking. | Involves both sides of the brain simultaneously. |
Understanding these differences is essential for UK medical teams to accurately map the tumour’s influence on the central nervous system.
Tumour Location and Seizure Patterns
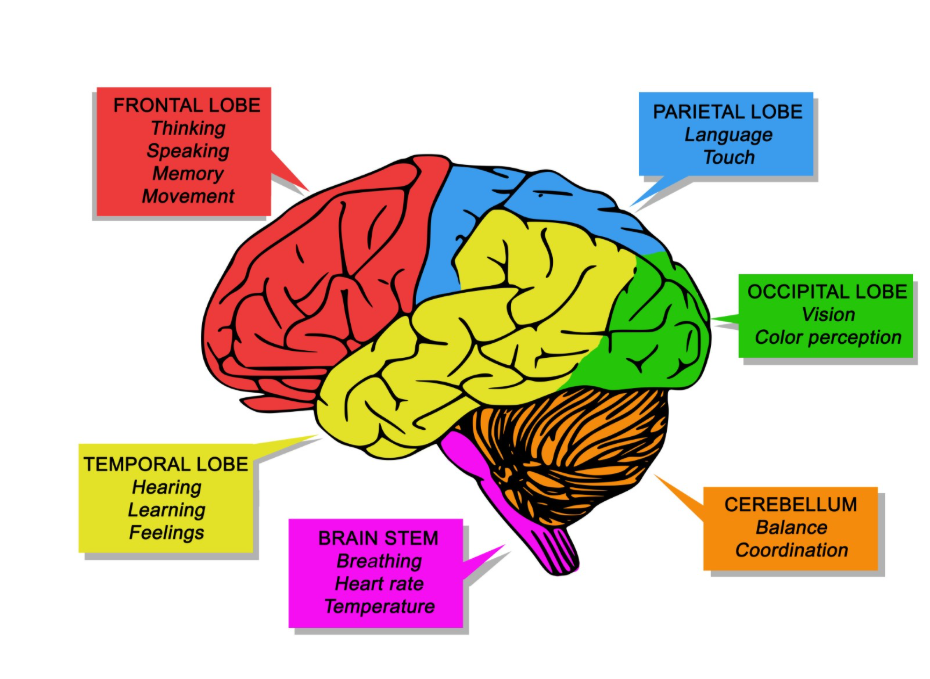
The specific part of the brain where a tumour is located dictates the symptoms of the seizure, as the electrical burst will affect the functions controlled by that area. For instance, a tumour in the motor cortex of the frontal lobe is highly likely to cause physical twitching or jerking on the opposite side of the body.

If the growth is in the temporal lobe, the seizure might involve “automatisms,” such as lip-smacking or picking at clothes, or sensory experiences like déjà vu. Occipital lobe tumours can trigger seizures that cause visual disturbances, such as flashing lights or temporary blindness. In the UK, specialists use the patient’s description of the seizure to help focus their imaging and neurological exams. Because some areas of the brain are more “epileptogenic” than others, certain tumours may be asymptomatic except for the occasional seizure. This relationship between anatomy and electrical activity is a cornerstone of the UK diagnostic process for intracranial growths.
Clinical Significance of First-Time Seizures
A first-time seizure in an adult with no history of epilepsy is regarded as a “red flag” symptom in the United Kingdom that necessitates an urgent referral for brain imaging. While many seizures are caused by metabolic issues, alcohol withdrawal, or high fevers, the possibility of a structural growth must be ruled out. The GOV.UK health pages provide clinical profiles that guide healthcare professionals in the urgent assessment of first-time seizures to ensure early detection of brain tumours.
When a patient presents to a UK emergency department or GP with a new seizure, they are usually referred for a CT or MRI scan. This rapid investigation is part of the UK’s commitment to the “28-Day Faster Diagnosis Standard.” Early identification of a tumour through seizure activity is often beneficial, as it allows for intervention before the tumour causes more extensive neurological damage or increases pressure within the skull to a dangerous level.
Management of Seizures in Tumour Patients
The management of seizures caused by a brain tumour in the UK involves a combination of anti-epileptic drugs (AEDs) and, in many cases, the physical removal of the tumour itself. AEDs work by stabilising the electrical activity of the nerve cells, making them less likely to fire abnormally.
If the seizures are caused by swelling around the tumour, steroids may also be used to reduce the inflammation and pressure. Often, the frequency and severity of seizures improve significantly after surgery to remove or shrink the growth. However, some patients may need to continue medication long-term to prevent further fits. In the United Kingdom, this care is coordinated by a multidisciplinary team including neurologists and neuro-oncologists. This team ensures that the medication does not interfere with other treatments and that the patient’s quality of life is maintained.
UK Clinical Pathways for Seizure Care
The United Kingdom uses integrated care pathways to ensure that patients with tumour-related seizures receive seamless support from diagnosis through to long-term recovery. This includes access to specialist nurses who can provide advice on living with seizures and the legal requirements regarding driving.
The UK pathway includes:
- Urgent Referral: Fast-tracked imaging for any adult with a new-onset seizure.
- Specialist Review: Assessment by a neurologist to confirm the seizure type and start medication.
- MDT Discussion: A group of experts determining the best surgical or monitoring plan.
- DVLA Coordination: Guidance on the mandatory reporting of seizures and brain tumours to the DVLA.
Following a seizure and a tumour diagnosis, UK law requires patients to stop driving and inform the DVLA. The clinical team provides the necessary documentation and support to help patients navigate these changes. This structured system ensures that the risks to the patient and the public are managed while providing a clear route back to normal life once the condition is stabilised.
Conclusion
A brain tumour can cause seizures by disrupting the electrical environment of the brain, often serving as one of the first identifiable symptoms of a growth. In the UK, a first-time seizure is treated as an urgent clinical sign requiring rapid imaging and specialist assessment. Management focuses on controlling the electrical activity with medication while addressing the underlying tumour through surgery or other therapies. Consistent clinical follow-up is essential for ensuring seizure control and neurological stability. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
If I have a seizure, does it definitely mean I have a brain tumour?
No; seizures have many causes, including epilepsy, infections, or head injuries, but in adults, a new seizure always requires investigation to rule out a tumour.
Can a small, benign tumour cause a big seizure?
Yes; the size of the tumour does not always match the severity of the seizure, as even a small growth can cause major electrical disruption in a sensitive area.
Will my seizures go away if the tumour is removed?
Many patients find their seizures improve or stop after surgery, but some may still require long-term medication to keep the electrical activity stable.
What should I do if I see someone having a seizure?
In the UK, the advice is to stay calm, clear the area of dangerous objects, time the seizure, and call 999 if it lasts longer than five minutes or is a first-time event.
Does the DVLA need to be told about my seizure?
Yes, in the UK, you must inform the DVLA of both a brain tumour and any seizure activity, as this will affect your driving licence.
Can stress trigger a seizure if I have a tumour?
While the tumour is the primary cause, factors like stress, lack of sleep, or alcohol can lower the “seizure threshold” and make a fit more likely.
Are there different medications for tumour-related seizures?
UK clinicians use several different anti-epileptic drugs, choosing the one that best suits the patient’s tumour type and other management plans.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding brain tumours and seizures, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in emergency care, neurosurgery, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


