


Surgery is not required for every brain tumour, as the necessity for an operation depends on the tumour type, its location, the presence of symptoms, and the overall health of the patient. In the United Kingdom, multidisciplinary teams evaluate each case to determine whether the benefits of surgical intervention outweigh the potential risks to healthy brain tissue. For some slow-growing or benign tumours, a strategy of active monitoring is often preferred over immediate surgery. Other tumours may be managed primarily through non-invasive therapies such as radiotherapy or medication. By adhering to evidence-based protocols established by the NHS and NICE, clinical teams ensure that surgical decisions are proportionate to the tumour behaviour and the needs of the individual. This article explores the clinical circumstances where surgery is essential and those where alternative management pathways are more appropriate within the UK healthcare framework.
What We’ll Discuss in This Article
- The role of active surveillance for slow-growing brain tumours.
- Circumstances where surgery is avoided due to high risk or location.
- Using radiotherapy and radiosurgery as alternatives to traditional surgery.
- Medical management of pituitary tumours through hormone therapy.
- The necessity of surgery for high-grade or symptomatic masses.
- How UK clinical teams coordinate non-surgical management plans.
Active Surveillance as a Non-Surgical Pathway
Active surveillance, frequently referred to as “watch and wait,” is a common non-surgical management strategy in the United Kingdom for small, slow-growing, or asymptomatic brain tumours. This approach is utilised when a tumour appears benign on imaging and is not currently causing pressure or neurological deficits. The NHS states that if a brain tumour is slow-growing and not causing symptoms, it may be monitored with regular scans rather than being treated immediately.
During this period, patients undergo scheduled MRI scans at set intervals to detect any changes in the size or characteristics of the mass. If the tumour remains stable, surgery can often be delayed indefinitely, allowing the patient to avoid the recovery time and risks associated with neurosurgery. This pathway is particularly common for Grade 1 meningiomas or small acoustic neuromas. In the UK, the decision to remain on surveillance is reviewed regularly by the multidisciplinary team. If growth is detected or symptoms emerge, the team will then re-evaluate the necessity of active treatment such as surgery or radiation.
When Surgery is Deemed High Risk
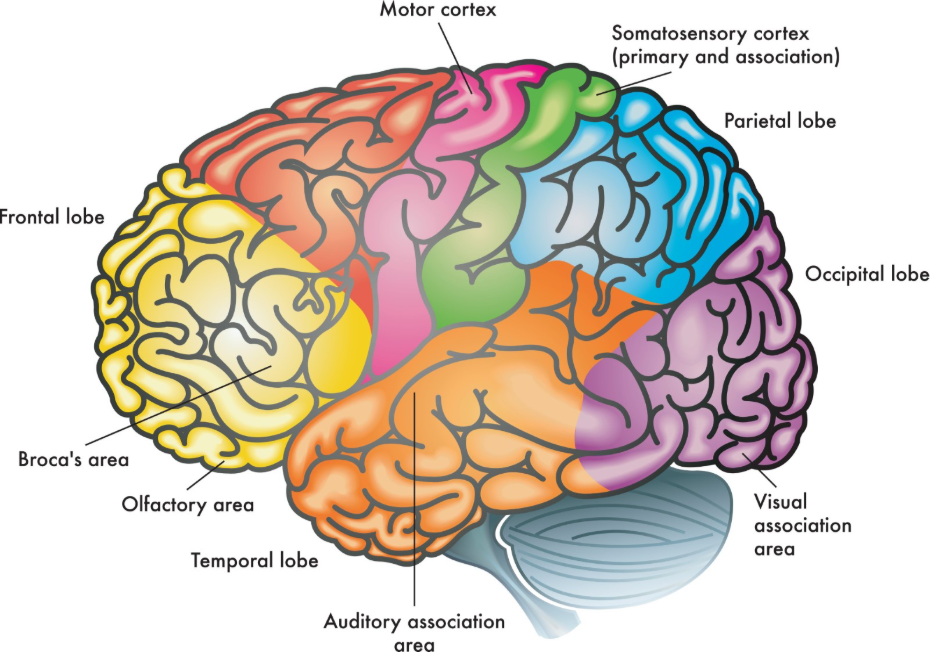
Surgery may be considered unnecessary or inappropriate if a brain tumour is located in an “eloquent” area or a deep-seated region where an operation would likely cause severe and permanent neurological damage. Eloquent areas are those parts of the brain responsible for vital functions such as speech, motor control, or vision. If a tumour is intertwined with critical blood vessels or the brainstem, a surgical attempt may carry a higher risk than the tumour itself.
In these clinical scenarios, UK specialists may prioritise:
- Targeted Radiotherapy: Managing the growth without physical intervention.
- Symptom Control: Using medication to address any effects of the mass.
- Preservation of Function: Avoiding surgery to maintain the patient’s current quality of life.
- Biopsy Only: Performing a minimally invasive procedure to confirm the cell type before starting non-surgical management.
NICE clinical guidelines for brain tumours indicate that for tumours in high-risk areas, the potential for neurological deficit must be carefully balanced against the goals of tumour removal. This patient-centred approach ensures that the management plan does not cause more harm than the condition. In the UK, neurosurgeons use advanced navigation and monitoring technology, but they will still recommend against surgery if the safety threshold cannot be met.
Radiotherapy and Radiosurgery as Primary Treatments
Radiotherapy and stereotactic radiosurgery serve as effective alternatives to traditional surgery for certain brain tumours, particularly those that are small, well-defined, or difficult to reach surgically. Stereotactic radiosurgery (SRS) delivers a single, highly concentrated dose of radiation to a precise target, effectively stopping the tumour from growing while sparing the surrounding healthy tissue.
| Treatment Type | Method | Common Use in UK |
| Traditional Surgery | Physical removal via craniotomy. | Large or high-grade symptomatic masses. |
| Radiosurgery (SRS) | Precise radiation without an incision. | Small, deep, or recurrent tumours. |
| Standard Radiotherapy | Multiple sessions of external radiation. | Post-surgery or for diffuse growths. |
In the United Kingdom, many patients with small acoustic neuromas or certain metastatic brain tumours are managed with radiosurgery rather than an operation. This non-invasive option allows for management in a single day without the need for a general anaesthetic or a hospital stay. While it does not physically remove the mass, the high-dose radiation causes the tumour cells to stop dividing, eventually leading to the mass shrinking or becoming inactive scar tissue. UK clinical teams use these technologies to provide safe alternatives for patients who may not be fit for surgery or whose tumours are better suited to radiological management.
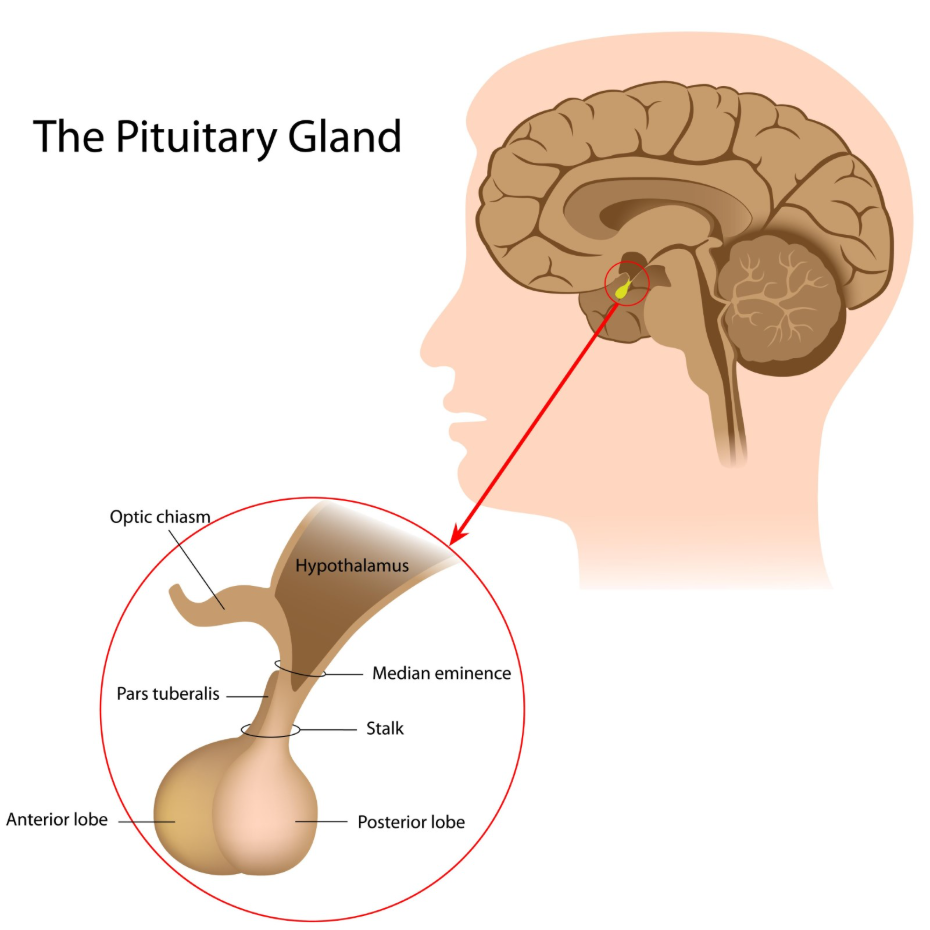
Medical Management of Hormone-Producing Tumours
Certain types of brain tumours, specifically those occurring in the pituitary gland, can often be managed entirely through medication without the need for surgery. Pituitary adenomas can cause health issues by overproducing hormones, such as prolactin, which can be effectively suppressed using specific drugs. The GOV.UK health pages provide clinical profiles indicating that for certain pituitary tumours, medical therapy can shrink the mass and normalise hormone levels as effectively as surgery.
For a prolactinoma, dopamine agonists are typically the first line of management in the UK. These medications can significantly reduce the size of the tumour and restore normal hormonal function. Surgery is generally reserved for cases where medication is not tolerated, is ineffective, or if the tumour is pressing on the optic nerves and threatening vision. This endocrine-led approach highlights how the biological characteristics of a tumour dictate whether an operation is truly necessary. UK multidisciplinary teams involve endocrinologists in these cases to ensure that all non-surgical pharmaceutical options are explored before considering a neurosurgical intervention.
When Surgery is Considered Essential
While many tumours do not require an operation, surgery is considered essential when a tumour is high-grade, causing significant pressure within the skull, or is resulting in rapidly worsening neurological symptoms. In these situations, the physical removal or “debulking” of the mass is required to save lives or prevent imminent neurological failure.
Surgery is typically mandatory for:
- High-Grade Gliomas: To reduce the number of cells and provide tissue for genetic analysis.
- Large Meningiomas: When they are causing significant “mass effect” and brain shift.
- Obstructive Hydrocephalus: If the tumour is blocking the flow of cerebrospinal fluid.
- Acute Deterioration: When a sudden change in symptoms requires immediate relief of pressure.
In the United Kingdom, the primary goal of surgery in these cases is to remove as much of the tumour as safely possible (maximal safe resection). This not only relieves symptoms but also makes subsequent treatments, such as radiotherapy or chemotherapy, more effective. Even if a total removal is not possible, debulking the mass can improve the patient’s quality of life and prolong the period of neurological stability.
Integrated Clinical Decision Making in the UK
The decision of whether surgery is necessary for a brain tumour is made through an integrated review process by a Multidisciplinary Team (MDT). This team brings together neurosurgeons, oncologists, radiologists, and specialist nurses to ensure that every diagnostic and treatment option is considered from multiple perspectives.
The UK MDT decision-making process involves:
- Imaging Review: Assessing the tumour’s growth rate and its proximity to eloquent brain regions.
- Symptom Correlation: Determining if the patient’s symptoms are directly caused by the mass.
- Risk Assessment: Evaluating the patient’s physical fitness for surgery and anaesthesia.
- Patient Preference: Discussing the goals of care and the acceptable level of risk with the individual.
Following this review, the team provides a unified recommendation. If surgery is not required, a clear alternative plan for surveillance or non-surgical treatment is established. This coordinated approach ensures that no patient in the UK undergoes an unnecessary or excessively risky operation. By centralising expertise, the NHS provides a robust framework for managing both the medical and surgical aspects of brain health, ensuring that interventions are always evidence-based and patient-centred.
Conclusion
Surgery is not necessary for every brain tumour and is often replaced by active surveillance, radiotherapy, or medical therapy depending on the clinical context. In the UK, the NHS prioritise non-surgical routes for stable, asymptomatic tumours and for those located in high-risk areas of the brain. However, surgery remains an essential and urgent intervention for high-grade tumours or those causing dangerous levels of intracranial pressure. Every management plan is tailored by a multidisciplinary team to ensure the best balance between tumour control and the preservation of neurological function. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a brain tumour disappear without surgery?
Primary brain tumours do not usually disappear on their own, but they can remain stable and inactive for many years under active surveillance.
What happens if I refuse surgery?
UK clinicians will discuss alternative options like radiotherapy or symptom management to ensure you receive the best possible care based on your choice.
Is radiosurgery the same as a traditional operation?
No; stereotactic radiosurgery uses precise radiation beams and does not involve an incision or a general anaesthetic.
Will my tumour grow while I am on “watch and wait”?
Some tumours remain the same size for years, while others may grow slowly; regular MRI scans are used to detect any changes early.
Are pituitary tumours always operated on?
No; many pituitary tumours are managed successfully with tablets that regulate hormones and shrink the mass.
How does a doctor decide if a tumour is “operable”?
A neurosurgeon assesses whether the tumour can be reached and removed without causing unacceptable damage to healthy brain tissue.
Can chemotherapy be used instead of surgery?
For some specific tumours, like certain lymphomas or germ cell tumours, chemotherapy may be the primary management, but for most, it is used after surgery.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the necessity of surgery for brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in general surgery, emergency care, and inpatient management. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


