


The selection of a treatment pathway for a brain tumour in the United Kingdom is a complex clinical process governed by the specific biological characteristics of the tumour and the individual health status of the patient. Doctors primarily evaluate the tumour grade, its precise anatomical location, and the presence of specific genetic markers to determine the most effective management strategy. In the UK, this decision is not made by a single physician but by a specialised multidisciplinary team (MDT) that integrates expertise from neurosurgery, oncology, and radiology. By following evidence-based protocols established by the NHS and NICE, these teams aim to balance the eradication of abnormal cells with the preservation of neurological function. Understanding the criteria used in this decision-making process helps patients and families navigate the complexities of their clinical journey within the UK healthcare system. This article explores the fundamental factors that influence treatment choices and how clinical teams coordinate care to achieve the best possible outcomes.
What We’ll Discuss in This Article
- The role of the World Health Organization (WHO) grading system.
- How the anatomical location of the tumour influences surgical options.
- The significance of molecular and genetic markers in modern oncology.
- Assessing patient fitness and overall health for intensive treatments.
- The collaborative role of the multidisciplinary team (MDT) in the UK.
- Balancing clinical effectiveness with the preservation of quality of life.
The Influence of WHO Tumour Grading
Doctors choose the intensity of a treatment plan based largely on the World Health Organization (WHO) grade assigned to the tumour, which indicates how aggressive the cells are and how quickly they are likely to grow. Grade 1 and 2 tumours are generally considered low-grade or slow-growing, while Grade 3 and 4 tumours are classified as high-grade or malignant. The NHS states that the grade of a brain tumour is a measure of how likely it is to grow or spread to other parts of the brain.
Low-grade tumours may sometimes be managed through active surveillance or surgery alone if the borders are well-defined. High-grade tumours require a more intensive, multi-modal approach that often includes surgery followed by radiotherapy and chemotherapy to address rapidly dividing cells. The grading system provides a standardised framework across the UK, ensuring that patients receive a level of intervention that is proportionate to the biological threat posed by the specific tumour type. Pathologists in the UK meticulously analyse tissue samples to confirm the grade before the MDT finalises the management strategy.
Anatomical Location and Surgical Feasibility
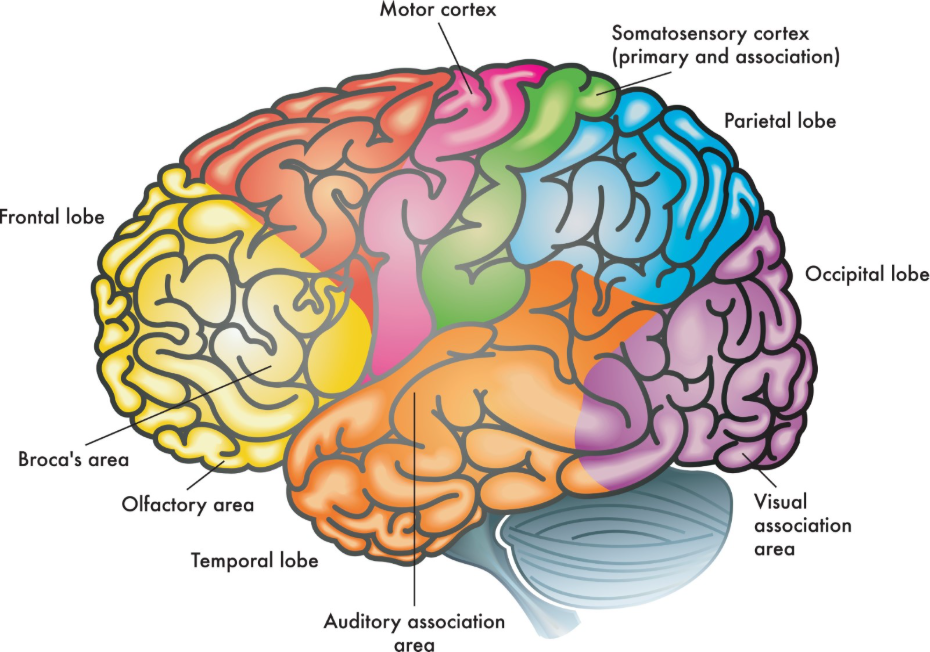
The location of a brain tumour is a critical factor in determining whether surgery is possible and what non-surgical alternatives, such as radiotherapy, should be considered. Doctors must assess if a tumour is located in an “eloquent” area of the brain parts responsible for vital functions like speech, motor control, or vision where surgery could cause permanent neurological damage.
| Location Category | Clinical Consideration | Typical Management Focus |
| Superficial / Accessible | Easier to reach via craniotomy. | Maximal safe surgical resection. |
| Deep-seated / Midline | Higher risk for traditional surgery. | Biopsy followed by radiation or SRS. |
| Eloquent Areas | Risk to speech, motor, or vision. | Mapping, awake surgery, or non-surgical routes. |
| Infiltrative | No clear border with healthy tissue. | Combined surgery and systemic therapy. |
NICE clinical guidelines for brain tumours indicate that the goal of surgery is maximal safe resection, which means removing as much of the tumour as possible without causing significant deficit. If a tumour is intertwined with critical blood vessels or located deep in the brainstem, the surgical risk may be deemed too high. In these cases, UK specialists may prioritise stereotactic radiosurgery or chemotherapy to manage the growth without a physical incision. This site-specific evaluation ensure that the chosen treatment does not inadvertently reduce the patient’s functional independence.
Molecular Markers and Personalised Medicine
In the United Kingdom, modern treatment selection is increasingly guided by molecular markers, which are specific genetic changes within the tumour cells that predict how they will respond to certain medications. These markers are identified through advanced genomic testing performed on the tissue sample obtained during a biopsy or operation. The GOV.UK health pages provide clinical profiles indicating that molecular markers are now essential for tailoring systemic treatments to the individual patient in the UK.
Key molecular factors include:
- MGMT Promoter Methylation: Predicts a better response to specific chemotherapy drugs.
- IDH Mutation Status: Helps distinguish between different types of gliomas and guides prognosis.
- 1p/19q Codeletion: Indicates a tumour type that is often more sensitive to combined therapy.
- BRAF Mutations: Found in some rare tumours and can be targeted with specific new drugs.
This information allows UK oncologists to move toward a more “personalised” approach, where chemotherapy or targeted therapies are only prescribed if the tumour’s genetic profile suggests they will be effective. This reduces the risk of patients being exposed to side effects from treatments that are unlikely to benefit their specific tumour subtype. By integrating genomic data into the decision process, the NHS ensures that the management plan is as precise as modern technology allows.
Assessing Patient Fitness and Performance Status
Doctors also consider the patient’s general physical fitness and “performance status” when choosing a treatment, as intensive options like major surgery or chemotherapy require a certain level of physiological resilience. A patient’s performance status is a clinical measure of their ability to perform daily activities and their level of independence.
For patients who have other serious health conditions, such as heart disease or significant respiratory issues, the risks of general anaesthesia for brain surgery may be unacceptably high. In these instances, the clinical team may recommend less invasive options like radiotherapy or hormone-blocking medications for pituitary tumours. In the UK, the focus is on providing care that is medically appropriate for the individual’s circumstances. This holistic assessment ensure that the treatment does not overwhelm the patient’s physical capacity to recover. The MDT carefully discusses these factors with the patient and their family to ensure that the chosen path aligns with the patient’s overall health goals.
The Role of the Multidisciplinary Team (MDT)
The final choice of treatment in the United Kingdom is a collaborative decision made by a Multidisciplinary Team (MDT) to ensure that all aspects of the patient’s condition are considered by experts. This team typically meets weekly and includes neurosurgeons, oncologists, neuroradiologists, neuropathologists, and specialist nurses.
The MDT review process ensures:
- Radiology Review: Assessing the latest scans to determine tumour size and location.
- Pathology Confirmation: Reviewing the microscopic and molecular results of the biopsy.
- Surgical Review: Deciding if a safe removal or debulking of the mass is possible.
- Oncology Planning: Determining the best sequence of radiotherapy or chemotherapy.
- Supportive Care: Ensuring that the patient’s physical and emotional needs are addressed.
This integrated approach acts as a safety net, ensuring that the diagnosis is accurate and that the treatment plan follows the latest evidence-based standards. By bringing together multiple specialities, the NHS provides a robust framework where complex cases benefit from a collective depth of expertise. Once the MDT reaches a consensus, the consultant discusses the recommended options with the patient, allowing for an informed and shared decision-making process.
Conclusion
Doctors in the UK choose brain tumour treatments by carefully weighing the tumour grade, anatomical location, and molecular profile against the patient’s overall health and functional goals. This complex evaluation is coordinated by multidisciplinary teams within the NHS to ensure that management is both effective and safe according to NICE standards. While high-grade tumours often require an intensive combination of surgery and oncology, low-grade or deep-seated masses may be managed with surveillance or targeted radiation. Every plan is designed to treat the tumour while protecting the patient’s neurological independence and quality of life. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
What is the most important factor in choosing treatment?
No single factor is most important; doctors look at the grade, location, and molecular markers together to decide the best path.
Can I ask for a second opinion in the UK?
Yes; you have the right to request a second opinion, although the MDT process already involves several specialists reviewing your case.
How does my age affect the treatment choice?
Age is considered alongside your general fitness; clinicians want to ensure you are strong enough for the side effects of certain treatments.
Why might my treatment be different from someone with the same tumour?
Differences in molecular markers or the exact location of the tumour in the brain can lead to different management plans.
Will my treatment plan change over time?
Yes; the plan is reviewed after each phase, such as surgery, and may be adjusted based on the latest scan results or biopsy findings.
Do doctors consider my personal wishes?
Absolutely; shared decision-making is a core part of the NHS, and your preferences regarding risks and quality of life are vital.
How long does the MDT take to decide?
MDT meetings happen weekly, and a recommendation is usually ready shortly after all your test and scan results are available.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the selection of brain tumour treatments, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in general surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


