


Long-term symptoms can persist after brain tumour treatment because the tumour itself or the interventions used to manage it, such as surgery and radiotherapy, can cause lasting changes to the delicate neural pathways of the brain. In the United Kingdom, healthcare professionals recognize that “recovery” often involves adapting to these persistent changes through integrated neurorehabilitation and specialist support. While many patients experience significant improvement over time, the complex nature of the central nervous system means that some physical, cognitive, or emotional effects may remain. The NHS follows evidence-based guidelines from NICE to provide a structured framework for long-term care and symptom management. Understanding the potential for persistent symptoms helps patients and families set realistic goals for the post-treatment phase. This article explores the common types of long-term effects, the factors that influence recovery, and the comprehensive support systems available within the UK healthcare framework to help individuals achieve the best possible quality of life.
What We’ll Discuss in This Article
- Common physical symptoms that may persist following treatment.
- The impact of treatment on long-term cognitive and memory function.
- Managing emotional health and personality changes after recovery.
- The role of neurorehabilitation in addressing permanent deficits.
- How radiotherapy and surgery contribute to late-onset effects.
- Integrated NHS support systems for long-term health and wellbeing.
Persistent Physical Symptoms and Mobility
Physical symptoms such as weakness, balance issues, or coordination difficulties can remain long after the primary treatment for a brain tumour is completed, especially if the tumour was located in motor-sensitive areas. These symptoms occur because the brain tissue responsible for physical movement may have been directly affected by the tumour or the surgical intervention. The NHS states that you may have some long-term problems after treatment, such as speech and language problems, or problems with your balance and coordination.
In the United Kingdom, physiotherapists work with patients to manage these lasting physical effects. While the brain has a degree of “plasticity,” meaning it can sometimes reorganize itself to bypass damaged areas, some deficits may be permanent. Common persistent physical issues include a loss of strength on one side of the body, reduced fine motor skills, or a continued risk of seizures. These are managed through a combination of regular exercise, specialist equipment, and anti-epileptic medications. By focusing on functional independence, the NHS helps patients adapt their lifestyle to accommodate these changes, ensuring they can safely perform daily activities despite any lingering physical challenges.
Cognitive Changes and Memory Function
Many patients in the United Kingdom experience long-term cognitive changes, such as difficulties with memory, attention, or information processing, which can impact their ability to return to work or manage complex tasks. These “hidden” symptoms are often the result of the brain’s delicate processing networks being disrupted by the presence of a tumour or the effects of radiotherapy on healthy brain cells. NICE clinical guidelines for brain tumours indicate that cognitive rehabilitation should be an integrated part of the long-term care plan for patients experiencing these persistent challenges.
Cognitive symptoms can manifest as:
- Short-term Memory Loss: Difficulty recalling recent conversations or appointments.
- Reduced Concentration: Struggling to focus on reading or complex projects for long periods.
- Executive Function Issues: Difficulty with planning, organizing, or multitasking.
- Information Processing Lag: Taking longer to understand and respond to new information.
Occupational therapists and neuropsychologists in the UK provide strategies to help patients manage these cognitive shifts. This might involve using digital memory aids, breaking down tasks into smaller steps, or establishing strict routines. Because these symptoms are not visible, they can sometimes be more frustrating for patients than physical disabilities. The UK healthcare system provides a framework for ongoing cognitive assessment to ensure that the support offered remains relevant as the patient’s recovery evolves.
Emotional Health and Behavioural Shifts
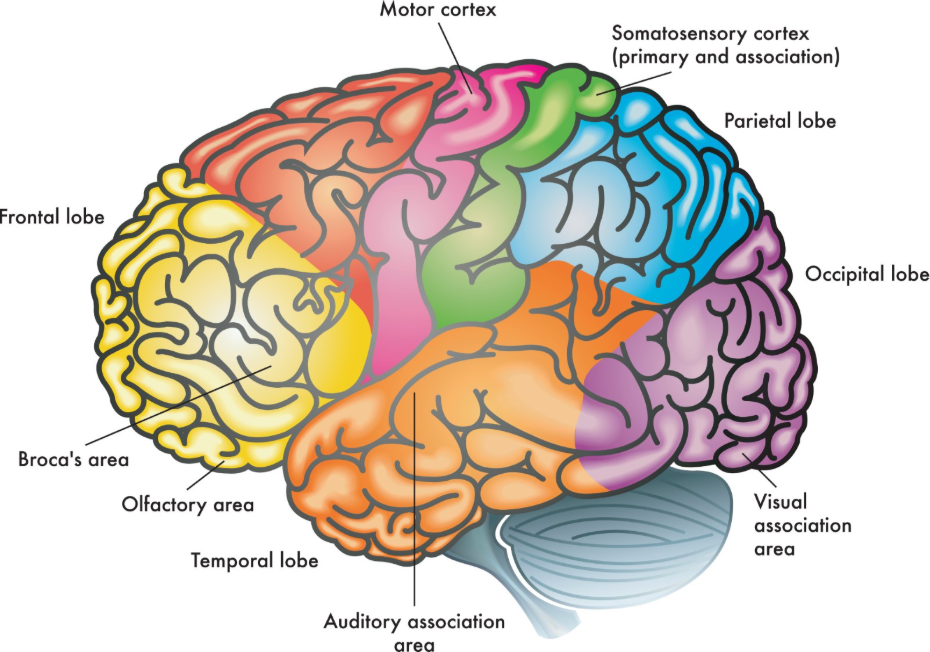
Long-term changes in emotional health, personality, or social behaviour can remain after treatment, particularly if the tumour involved the frontal lobes, which act as the brain’s control centre for mood and social conduct. Patients may find that they become more easily frustrated, experience mood swings, or feel a general sense of “flatness” or apathy.
| Symptom Category | Potential Long-term Change | Clinical Support in UK |
| Mood | Increased anxiety or depression. | Clinical psychology and counselling. |
| Personality | Shifts in social inhibition or motivation. | Neuropsychology and family support. |
| Fatigue | Persistent, overwhelming tiredness. | Energy pacing and specialist nurse guidance. |
| Social | Difficulty with social interactions. | Speech therapy and peer support groups. |
In the United Kingdom, these changes are managed through integrated psychological support and family-centred care. It is common for the patient’s family to notice these shifts first, and the NHS provides resources to help everyone adjust to the “new normal.” Clinical psychologists work with patients to develop coping mechanisms for emotional regulation, while specialist nurses (key workers) provide a consistent link to medical advice. Acknowledging that emotional recovery takes as much time as physical healing is a vital part of the long-term management strategy in the UK.
Late Effects of Surgery and Radiotherapy
Some symptoms may not appear immediately but can develop months or even years after treatment has finished; these are known as “late effects” and are often associated with the long-term impact of radiotherapy or extensive surgery. Radiotherapy works by damaging the DNA of tumour cells, but it can also cause gradual changes to the surrounding healthy brain tissue and small blood vessels over time. The GOV.UK health pages provide clinical profiles indicating that long-term monitoring for late effects of treatment is a mandatory part of the follow-up pathway in the UK.
Late effects can include:
- Endocrine Issues: Changes in hormone production if the pituitary gland was near the treatment area.
- Cognitive Decline: A gradual shift in memory or thinking skills years after radiation.
- Visual Changes: Occurring if the optic nerves were within the treatment field.
- Radiation Necrosis: A rare late-term reaction where dead tissue causes inflammation and symptoms similar to a tumour.
Because of the potential for these delayed symptoms, the UK healthcare system implements a lifetime of surveillance for many patients. Regular MRI scans and clinical reviews ensure that if late effects do occur, they are identified and managed promptly. This long-term vigilance is a hallmark of UK clinical practice, recognizing that the journey with a brain tumour does not end when the initial treatment finishes.
The Role of Neurorehabilitation in Recovery
Neurorehabilitation is the primary framework used in the United Kingdom to help patients manage and improve persistent symptoms after brain tumour treatment. This integrated service brings together various specialities to support the patient’s functional recovery and to help them adapt to any permanent deficits.
The UK rehabilitation team typically involves:
- Physiotherapists: Focusing on physical strength, gait, and balance.
- Occupational Therapists: Assisting with daily tasks, home safety, and returning to work.
- Speech and Language Therapists: Supporting communication and swallowing function.
- Neuropsychologists: Assessing cognitive health and providing emotional support.
Rehabilitation is most effective when it is started early and continued as long as the patient is making progress toward their functional goals. In the UK, these services are provided both in hospital and through community-based teams. The goal is to maximize the patient’s independence and to provide them with the tools they need to live as full a life as possible. This supportive care is adjusted over time as the patient’s needs change, providing a continuous safety net throughout the recovery process.
Integrated NHS Support and Follow-up Care
Long-term care for patients in the United Kingdom is coordinated by multidisciplinary teams to ensure that all persistent symptoms are monitored and that the patient has access to consistent medical oversight. This follow-up care is essential for detecting any changes in the tumour site and for managing the ongoing physical and emotional needs of the individual.
The UK follow-up pathway ensures:
- Scheduled MRI Scans: Monitoring the brain for any signs of regrowth or late effects.
- Clinical Reviews: Regular appointments with a consultant or specialist nurse.
- Symptom Tracking: Encouraging patients to report any new or worsening signs.
- Social Care Liaison: Arranging for home support or equipment if needed.
Specialist nurses, or key workers, play a vital role in this integrated system, acting as the main point of contact for the patient and their family. They provide a vital link between the different specialities and ensure that the care remains patient centred. By providing this structured long-term framework, the NHS supports individuals in managing the complexities of life after a brain tumour, focusing on both clinical safety and personal wellbeing.
Conclusion
Long-term symptoms can remain after brain tumour treatment due to the impact of the growth and the therapies on the brain’s complex neural networks. In the UK, the NHS provides an integrated pathway of neurorehabilitation involving physiotherapists, occupational therapists, and neuropsychologists to help patients manage these persistent changes. While some effects on memory, movement, or mood may be permanent, many improve over time with specialist support and adaptive strategies. Late effects of treatment are monitored through a structured follow-up programme to ensure any changes are addressed promptly. Every patient’s recovery is unique and is managed by a multidisciplinary team to ensure the best possible quality of life. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why do I still feel so tired months after my treatment has finished?
Post-treatment fatigue is very common and is the body’s response to the intense process of healing; it often requires a slow, “paced” return to activity.
Will my memory ever fully go back to how it was before?
For many, memory improves over time, but some may need to use compensatory strategies like diaries or alerts as a permanent way to manage.
Can seizures start for the first time after treatment is over?
Yes; scar tissue from surgery or radiotherapy can occasionally cause seizures to develop later, which is why UK doctors monitor you closely.
What is “brain fog” and how long does it last?
Brain fog is a common term for cognitive slowness or confusion; it usually improves gradually over several months as the brain recovers.
Are personality changes permanent?
Some behavioural shifts can be permanent if specific brain regions were damaged, but many emotional changes improve with specialist support and time.
How can a speech therapist help if I can speak but just forget words?
Speech therapists specialize in “word-finding” strategies and can help you develop techniques to recall information more effectively.
Can I still have rehabilitation years after my surgery?
Yes; if you develop new needs or if your function changes, your GP in the UK can refer you back to the neuro-rehabilitation team for a review.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding persistent symptoms after brain tumour treatment, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery, cardiology, emergency medicine, and psychiatry. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


