

Colon polyps and diverticulitis typically begin to appear more frequently as individuals reach the age of 50 and above, representing a common aspect of the biological ageing process of the digestive tract. While both conditions involve structural changes to the large intestine, they are driven by different physiological mechanisms: polyps are cellular overgrowths on the inner lining, whereas diverticulitis involves the inflammation of small pouches that bulge outward from the colon wall. In the United Kingdom, healthcare professionals monitor these conditions closely through national screening programmes and clinical assessments because their prevalence increases significantly with each decade of life. Although it is possible for these conditions to develop in younger adults, especially in cases involving specific genetic predispositions or significant lifestyle factors, they are primarily associated with the long-term wear and tear on the bowel. Understanding the typical age of onset is essential for ensuring that patients participate in timely screening and recognise early symptoms. By identifying these changes as they emerge, the UK healthcare system can manage risks effectively and maintain the functional health of the gastrointestinal system throughout a person’s later years.
What We’ll Discuss in This Article
- The typical age range for the development of colon polyps.
- Why diverticulosis and diverticulitis become more common after age 50.
- Biological factors that contribute to age-related bowel changes.
- The impact of genetics and lifestyle on earlier symptom onset.
- UK clinical guidelines for the start of national bowel screening.
- Monitoring protocols for maintaining colon health as the body ages.
Typical Age for the Development of Colon Polyps
Colon polyps most commonly begin to be detected in adults aged 50 and over, which is why UK national screening programmes are strategically targeted toward this age group. A polyp is a small growth of excess tissue on the inner lining of the colon that forms when the natural cycle of cell death and renewal is disrupted. The NHS states that bowel polyps are very common, especially as you get older, and affect around 1 in 4 people aged 50 or over.
While the majority of these growths remain benign, the risk of a polyp undergoing cellular changes that could lead to cancer increases with age. Because these growths are often silent and do not cause pain, they are usually found during routine screening tests or colonoscopies performed for other reasons. In the United Kingdom, the identification and removal of polyps in individuals during their 50s and 60s is a primary preventative measure. By clearing these growths early, clinicians interrupt the slow biological timeline that could otherwise lead to more serious gastrointestinal conditions in later decades.
Onset of Diverticulosis and Diverticulitis
Diverticulosis, the presence of small pouches in the colon wall, is exceptionally common in older age, with diverticulitis flare-ups typically appearing after the age of 40 and becoming increasingly prevalent by age 70. Diverticula form when high pressure within the bowel pushes the inner lining through weakened spots in the muscular layer of the colon. The NHS explains that diverticular disease and diverticulitis are more common as people get older, with many people having some diverticula by the time they reach 50.
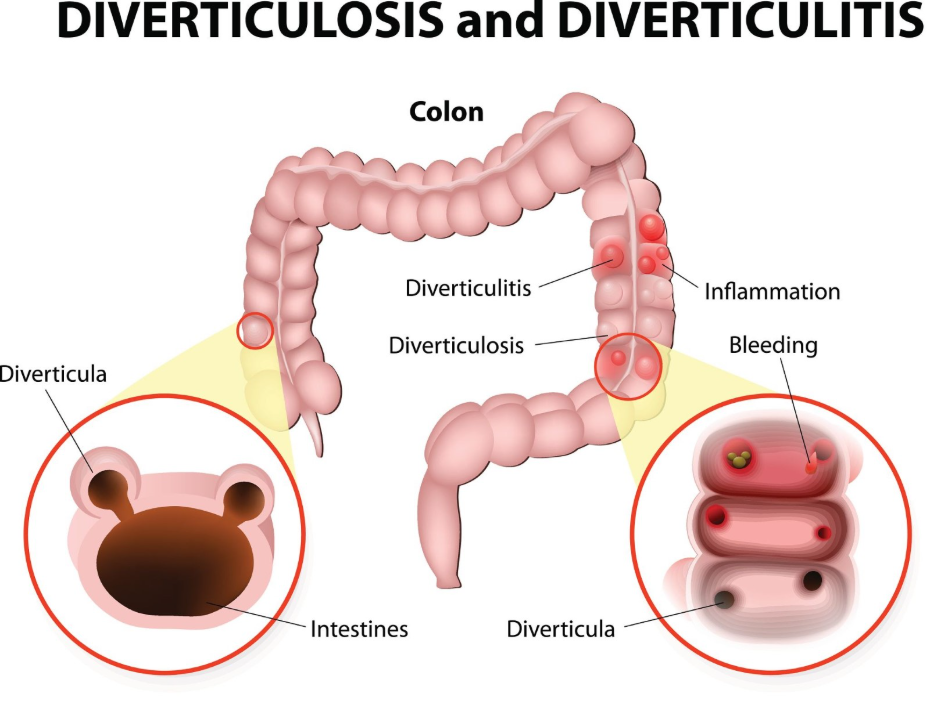
While the presence of these pouches (diverticulosis) is often asymptomatic, diverticulitis occurs when a pouch becomes infected or inflamed, leading to acute abdominal pain. In the UK, it is estimated that a significant portion of the population will have developed these structural changes by their 70th year. The age of onset for diverticular disease is closely linked to the long-term effects of low-fibre diets and the natural loss of elasticity in the bowel wall that occurs as the body ages. Clinicians manage these cases by focusing on symptom relief during acute episodes and providing long-term dietary advice to support the weakened bowel structure.
Biological Factors Contributing to Age-Related Changes
The reason polyps and diverticula appear more frequently in later life is rooted in the cumulative impact of cellular mutations and the progressive weakening of the connective tissues in the colon. As the body ages, the genetic mechanisms that regulate cell division can become less efficient, allowing small clusters of cells to grow into polyps. Simultaneously, the muscular wall of the large intestine becomes less resilient, making it more susceptible to the internal pressures that create diverticula.
In the United Kingdom, healthcare professionals view these changes as part of the “wear and tear” associated with decades of processing waste. The colon must move contents through its length using muscular contractions; over time, the stress of this process, particularly if stools are consistently hard or small, can lead to the structural protrusions seen in diverticular disease. Because these biological changes take many years to manifest into visible symptoms or detectable growths, they are rarely seen in children or young adults unless there is an underlying hereditary condition. This slow progression is why age remains the most significant non-modifiable risk factor for both conditions in the UK population.
Onset in Younger Adults and Risk Factors
While polyps and diverticulitis are primarily associated with older age, they can appear in younger adults due to genetic predispositions or modifiable lifestyle factors like obesity and diet. Hereditary conditions such as Lynch syndrome or familial adenomatous polyposis can cause polyps to develop as early as the teenage years or early 20s. Similarly, cases of diverticulitis in adults under the age of 40 have been noted more frequently in the UK in recent years, often associated with higher Body Mass Index and low-fibre intake.
| Feature | Typical Onset (50+) | Early Onset (Under 40) |
| Primary Driver | Natural ageing and long-term diet. | Often genetics or significant obesity. |
| Detection Method | Routine national screening. | Symptom-led investigation. |
| Polyp Risk | Cumulative over decades. | Higher risk of recurrence if genetic. |
| Diverticulitis | Common; often uncomplicated. | Can be more severe in younger patients. |
In the UK, if a younger individual presents with symptoms such as persistent rectal bleeding or severe lower left abdominal pain, clinicians do not rule out these conditions based on age alone. NICE clinical guidelines for colorectal cancer state that any unexplained change in bowel habits or rectal bleeding should be investigated regardless of age, especially if there is a family history of bowel conditions. Recognising that these conditions can occasionally deviate from the typical age of onset ensures that younger patients receive the necessary diagnostic care, such as a colonoscopy or genetic testing.
UK National Bowel Screening and Age Thresholds
The UK national bowel screening programme is designed to detect polyps and early signs of bowel disease by inviting individuals to participate starting from specific age thresholds. Currently, the programme typically begins inviting adults from age 50 or 60, depending on the specific region in the UK, with the goal of identifying polyps when they are most likely to begin appearing.
Participants are asked to provide a stool sample using a home test kit, which looks for microscopic amounts of blood. If blood is detected, it may be a sign of polyps or diverticular bleeding, prompting a follow-up colonoscopy. The GOV.UK health pages indicate that screening at these specific age intervals is the most effective way to identify high-risk growths and reduce the long-term incidence of bowel cancer. By aligning the start of screening with the typical biological onset of these conditions, the NHS ensures that interventions occur at a stage where polyps can be easily removed and diverticular health can be monitored.
Long-term Monitoring as the Body Ages
As individuals move into their 60s, 70s, and beyond, regular monitoring of bowel health becomes a standard part of clinical care to manage the high prevalence of both polyps and diverticular disease. For those with known diverticula, clinicians focus on preventing diverticulitis flare-ups through dietary management and hydration. For those who have had polyps removed, a surveillance schedule is established to check for new growths at regular intervals.
This ongoing oversight is necessary because the environment of the colon remains susceptible to the same factors that caused the initial changes. In the UK, integrated care pathways involve general practitioners, endoscopists, and dietitians to support patients in maintaining soft stools and a healthy mucosal lining. While age increases the likelihood of these conditions appearing, proactive management—including participation in all offered screenings—allows most people to manage these structural changes effectively. By understanding that these issues are a common part of the ageing process, patients can work with their healthcare teams to ensure that any new developments are caught early and treated with conservative or procedural measures as appropriate.
Conclusion
Colon polyps and diverticulitis typically begin to appear with greater frequency once individuals reach age 50, reflecting the natural ageing and long-term stress on the bowel wall. While polyps are often silent cellular overgrowths, diverticulitis is an inflammatory condition that causes acute pain, both of which become more prevalent in later life. In the UK, national screening and clinical monitoring are targeted toward these age groups to ensure early detection and management. Maintaining a high-fibre diet and participating in all health screenings are the best ways to protect colon health as the body ages. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can I get polyps in my 20s or 30s?
It is rare, but polyps can occur in younger people, particularly if there is a family history of bowel conditions or certain genetic syndromes.
Why does age 50 seem to be the turning point for bowel health?
Decades of processing waste and the natural loss of tissue elasticity mean that by age 50, structural changes like polyps and diverticula are much more likely to be present.
Do I still need to screen if I have no symptoms at age 60?
Yes, because polyps and early bowel changes rarely cause symptoms, screening is the only way to find them while they are small and easy to treat.
Does diverticulitis always happen after age 70?
No, while common in the elderly, many people have their first flare-up in their 40s or 50s, especially if they have a low-fibre diet.
Will a colonoscopy show both polyps and diverticula?
Yes, a colonoscopy allows a doctor to see the entire inner lining of the colon and identify both inward growths and outward pouches.
Can a healthy diet delay the appearance of these conditions?
A high-fibre diet can significantly reduce the pressure in the colon, which may delay or prevent the formation of diverticula and support a healthy bowel lining.
Is it normal to have both polyps and diverticula at age 65?
Yes, it is very common for older adults in the UK to have both conditions simultaneously as they are both results of the ageing process in the colon.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the typical age of onset for colon polyps and diverticulitis, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine, general surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
