What reproductive options exist for carriers of muscular dystrophy genes in the UK?
For individuals in the UK who carry genes for muscular dystrophy, there are several medical pathways available to help manage the risk of passing the condition to future generations. Advances in genetic medicine have expanded the range of reproductive choices, allowing prospective parents to make informed decisions based on their personal values and clinical circumstances. These options are provided through specialized NHS genetic services and fertility clinics, ensuring that families receive both technical expertise and psychological support throughout the process. Understanding these pathways is a fundamental part of family planning for known carriers of Duchenne, Becker, or other forms of muscular dystrophy.
What We’ll Discuss in This Article
- The role of genetic counselling in exploring reproductive choices.
- Pre-implantation genetic testing for monogenic disorders (PGT-M).
- Prenatal diagnostic testing options during pregnancy.
- The use of donor eggs or embryos as an alternative pathway.
- Non-invasive prenatal clinical screening and its limitations.
- Navigating NHS funding and specialist fertility referrals in the UK.
The role of genetic counselling in family planning
The first step for any carrier exploring reproductive options in the UK is a referral to a regional genetic service for specialist counselling. Genetic counsellors help individuals and couples understand the specific inheritance pattern of their condition, such as X-linked, autosomal dominant, or autosomal recessive, and calculate the statistical risk for future children. The NHS provides clinical genetics services to help people understand how their family history might affect their health and the health of their children. This service ensures that prospective parents have a clear, factual foundation before deciding which medical pathway, if any, they wish to pursue.
During these consultations, the counsellor explains the technical aspects of the various tests and the emotional implications of each choice. The process is non-directive, meaning the healthcare professional provides the information but respects the couple’s right to make their own decision. This support is particularly important because the journey through assisted reproduction or prenatal testing can be complex and requires a high level of informed consent. Counselling also addresses the potential impact of these decisions on the wider family, as genetic information often has relevance for siblings and other relatives.
Pre-implantation Genetic Testing for Monogenic disorders (PGT-M)
Pre-implantation genetic testing for monogenic disorders, formerly known as PGD, is a highly specialized IVF procedure that allows embryos to be screened for a specific muscular dystrophy mutation before they are transferred to the womb. This process involves creating embryos in a laboratory through In Vitro Fertilisation (IVF) and then removing a few cells from each embryo for genetic analysis. Only embryos that do not carry the specific mutation or are unaffected carriers are selected for implantation.
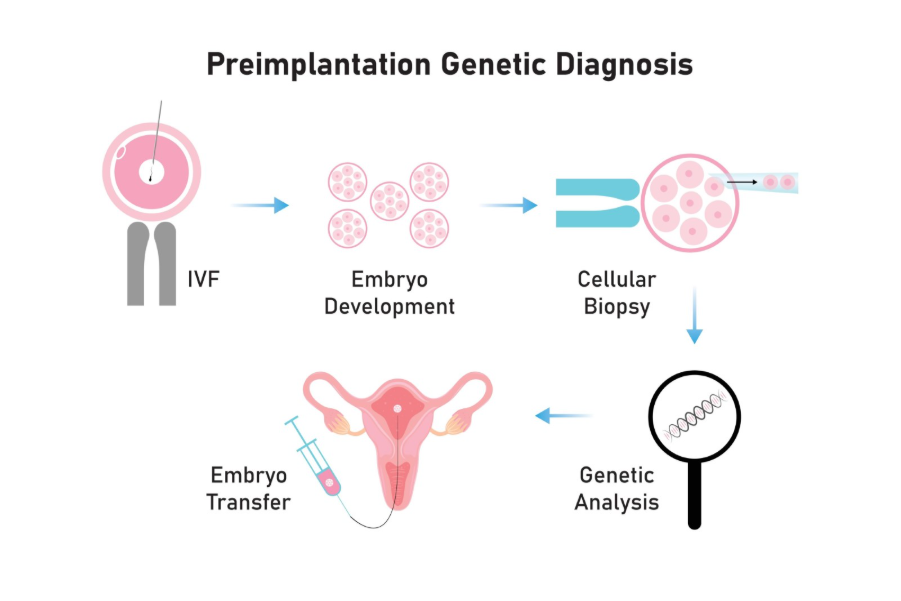
Shutterstock
NICE guidelines recommend that individuals with a known high risk of transmitting a serious genetic condition should have access to specialist genetic and fertility services to discuss PGT-M. In the UK, this treatment is strictly regulated by the Human Fertilisation and Embryology Authority (HFEA). For many carriers, PGT-M is a preferred option because it avoids the difficult decision of whether to continue a pregnancy if the fetus is found to be affected later on. However, it is a physically and emotionally demanding process with no guarantee of a successful pregnancy, and eligibility for NHS funding depends on specific criteria, such as not already having unaffected children.
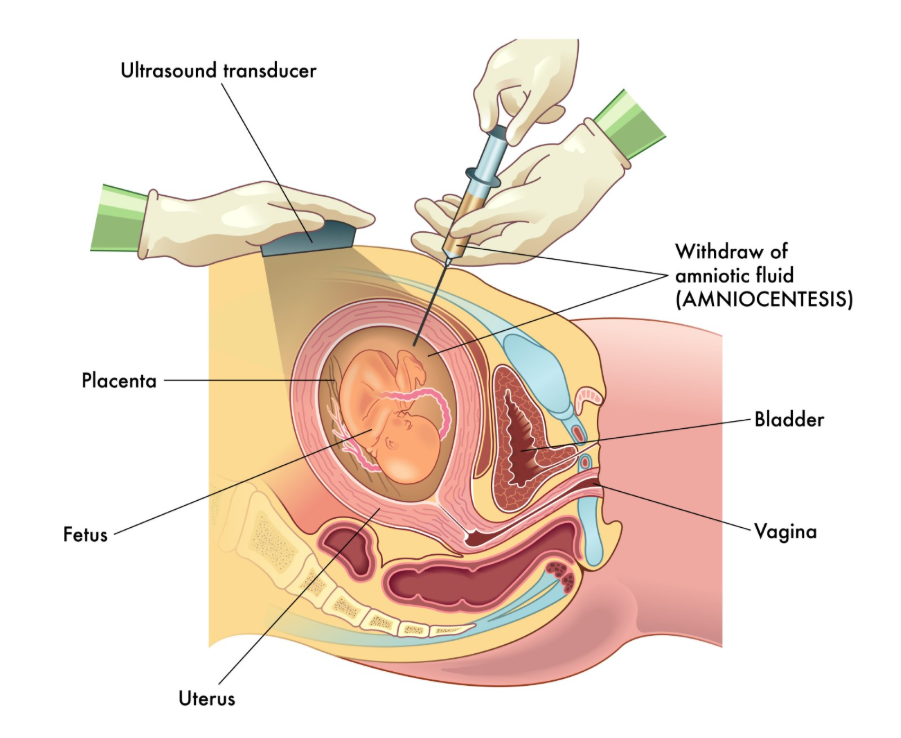
Prenatal diagnostic testing during pregnancy
Prospective parents who conceive naturally can opt for prenatal diagnostic tests, such as chorionic villus sampling (CVS) or amniocentesis, to determine if the fetus has inherited the muscular dystrophy gene. CVS is typically performed between the 11th and 14th weeks of pregnancy and involves taking a small sample of tissue from the placenta. Amniocentesis is usually carried out after the 15th week and involves testing a sample of the fluid surrounding the baby. Both tests provide a definitive result but carry a small risk of miscarriage, which is discussed in detail during the consent process.
If the results show that the fetus is affected by muscular dystrophy, the parents are supported by their genetic and obstetric teams to discuss their options. This may include continuing the pregnancy and preparing for the child’s needs or choosing to terminate the pregnancy. In the UK, these decisions are handled with a high degree of clinical sensitivity and privacy. For some conditions, such as Duchenne muscular dystrophy, non-invasive prenatal testing (NIPT) can sometimes be used to determine the sex of the fetus from a maternal blood sample early in pregnancy, which can help decide if further invasive testing is necessary.
Using donor eggs or embryos
Using donor eggs or donor embryos is an alternative reproductive option that entirely removes the risk of passing on the carrier’s specific genetic mutation. This pathway involves using eggs provided by a donor who does not carry the muscular dystrophy gene, which are then fertilized with the partner’s sperm (or donor sperm) and transferred to the carrier’s womb. While the resulting child will not be genetically related to the mother, this option allows the carrier to experience pregnancy and childbirth while ensuring the child is free from the condition.
| Option | Method | Key Benefit | Main Consideration |
| PGT-M (with IVF) | Embryo screening before pregnancy. | Prevents passing the gene; no termination needed. | Low success rates per cycle; physically demanding. |
| Prenatal Testing | Testing during natural pregnancy. | Can conceive naturally; high accuracy. | Risk of miscarriage; may involve difficult choices. |
| Donor Eggs | IVF using non-carrier eggs. | Eliminates genetic risk; pregnancy possible. | No genetic link to the mother; involves donors. |
| Adoption | Legal process to become a parent. | Provides a home to a child; no medical risk. | Lengthy legal process; no biological link. |
Export to Sheets
In the UK, egg donation is a regulated and altruistic process. Fertility clinics provide thorough screening for donors to ensure they are healthy and do not carry known genetic disorders. Choosing this path involves significant psychological preparation, and clinics provide mandatory implications counselling to help couples navigate the long-term aspects of donor conception. This option is often considered by individuals who have had unsuccessful PGT-M cycles or those who prefer to avoid the complexities of genetic testing altogether.
Accessing NHS funding and specialist referrals
Eligibility for NHS-funded reproductive options like PGT-M is governed by specific clinical criteria and varies depending on the local Integrated Care Board (ICB) in England or the equivalent health boards in Scotland, Wales, and Northern Ireland. Generally, couples must be at a high risk of having a child with a serious condition and must not have any living, unaffected children from their current relationship. There are also requirements regarding maternal age, body mass index (BMI), and non-smoking status that must be met to qualify for funded cycles.
The process begins with the GP or a specialist neurologist referring the patient to a regional genetics centre. Once the genetic risk is confirmed, the genetics team can then refer the couple to a licensed PGT-M centre for a fertility assessment. Because these treatments are specialized and expensive, the pathway can involve several stages of administrative and clinical approval. For those who do not meet the NHS criteria, self-funding at a private fertility clinic is an alternative, though the costs of IVF combined with genetic screening are substantial.
Conclusion
Reproductive options for muscular dystrophy carriers in the UK range from pre-implantation genetic testing and prenatal diagnosis to the use of donor eggs or adoption. Each pathway offers a different balance of clinical certainty, physical demand, and ethical considerations. The NHS provides a robust framework of genetic counselling and specialist fertility care to ensure that carriers can explore these options in a safe and supportive environment. Decisions regarding family planning are deeply personal, and the goal of the UK health system is to provide the information and technology needed to help families make the best choice for their future.
Is PGT-M available for all types of muscular dystrophy?
It is available for most types where the specific gene mutation has been identified, but the HFEA must approve the condition for testing in the UK.
Does PGT-M guarantee a healthy baby?
While highly accurate at identifying the mutation, PGT-M does not guarantee a pregnancy or rule out other unrelated health conditions or chromosomal issues.
Can I get PGT-M on the NHS if I already have a child with MD?
In many parts of the UK, you may be eligible for NHS funding if you have an affected child but no unaffected children, though local policies can vary.
How accurate is prenatal testing like CVS?
CVS and amniocentesis are diagnostic tests with an accuracy rate of over 99% for detecting the specific genetic mutation they are testing for.
Is there a waiting list for genetic counselling?
Wait times vary by region, but once a referral is made, the genetics service will prioritize cases based on the urgency of the reproductive or clinical situation.
What is the maximum age for NHS-funded IVF/PGT-M?
Most NHS boards in the UK set an upper age limit for the mother, typically around 39 or 40, to ensure the best chance of a successful outcome.
Can I use NIPT to screen for muscular dystrophy?
Non-invasive prenatal testing (NIPT) is currently used primarily for sex determination in X-linked conditions; it is not yet a standard diagnostic tool for the mutation itself.
Authority Snapshot
This article provides evidence-based information on reproductive options, strictly adhering to the clinical and safety standards of the NHS and NICE. The content has been reviewed by Dr. Stefan Petrov, a UK-trained physician with extensive experience in general medicine, surgery, and emergency care. Dr. Petrov’s clinical background ensures that this guide accurately reflects the regulatory and diagnostic pathways available within the UK health system for genetic carriers.
