Are MRI scans useful for osteoarthritis?
While MRI scans provide an incredible level of detail regarding the internal structures of a joint, they are rarely needed for the routine diagnosis of osteoarthritis. Most cases can be identified through a physical examination and a review of symptoms, as the hallmark changes of the condition, such as cartilage thinning and bone spurs, are often better evaluated through other means. MRI technology is primarily designed to visualise soft tissues like ligaments, tendons, and the meniscus, making it a powerful tool when a doctor suspects an injury other than simple joint wear. Understanding the specific utility of an MRI can help you navigate the diagnostic process with your general practitioner and ensure that imaging is used only when it will significantly change your management plan.
What We’ll Discuss in This Article
- The clinical difference between MRI and X-ray imaging
- When an MRI is necessary for atypical osteoarthritis symptoms
- How MRI scans help identify soft tissue injuries like meniscal tears
- The role of MRI in detecting early inflammation and fluid build-up
- Why MRI is not a routine requirement for starting a management plan
- Identifying triggers that might lead a professional to request an MRI
- Differentiating between structural wear and acute soft tissue damage
What an MRI sees that an X-ray misses
An MRI uses powerful magnets and radio waves to create a detailed map of all the tissues within a joint, not just the bone. Unlike a standard X-ray, which only shows the indirect signs of cartilage thinning, an MRI provides a direct view of the articular cartilage. This allows doctors to see the exact thickness and identify any surface irregularities or cracks that are occurring.
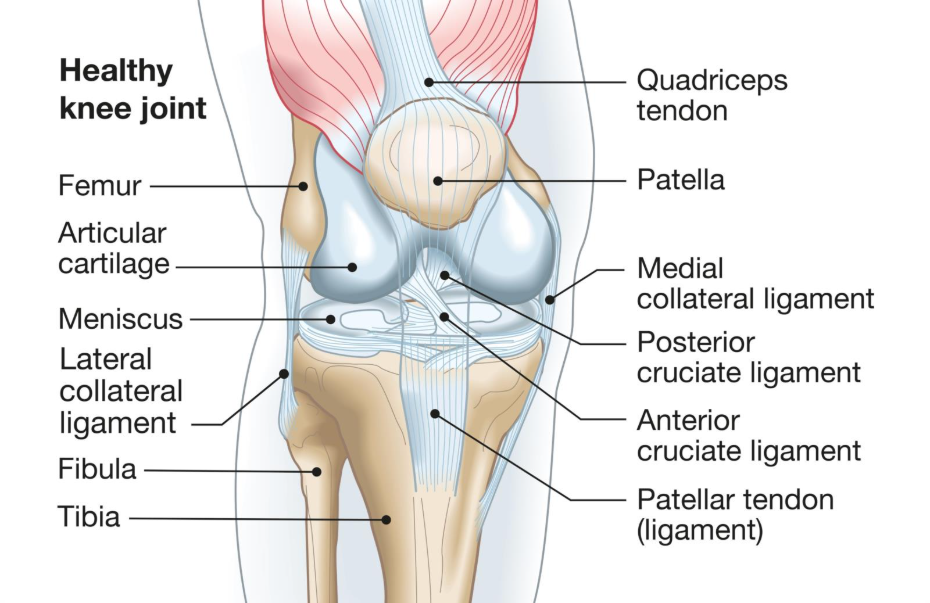
Furthermore, the MRI is excellent for visualising the soft tissues that provide stability and cushioning. It can identify issues with the meniscus, such as tears or fraying, and reveal the health of the ligaments and tendons. It can also detect early signs of inflammation in the joint lining or bone marrow oedema, swelling within the bone, which are not visible on any other type of scan. While this detail is impressive, it is often more than is needed for a standard ‘wear and repair’ diagnosis.
When an MRI is medically useful
Although a clinical diagnosis is standard, there are certain scenarios where an MRI is the most appropriate next step for a general practitioner.
- Diagnostic Uncertainty: If your symptoms do not follow the typical pattern, an MRI can help rule out other causes of pain.
- Atypical Symptoms: If the joint pain is constant, occurs at rest, or is accompanied by significant swelling, more detail may be needed.
- Joint Locking: If your joint frequently ‘catches’ or locks in place, an MRI is excellent for finding loose fragments of bone or cartilage.
- Suspected Soft Tissue Injury: If the pain follows a specific traumatic event, such as a sharp twist or fall, the doctor may need to check for a torn ligament.
In these cases, the MRI provides specific answers that an X-ray or a physical exam cannot provide, helping to ensure that the correct treatment is started.
The limitations of MRI for osteoarthritis
Despite its high level of detail, an MRI is not always the best tool for managing osteoarthritis due to several practical and clinical factors. One significant issue is ‘over-diagnosis’. Because an MRI is so sensitive, it often shows minor changes, like small meniscal tears, that are actually a normal part of ageing and are not the cause of the person’s pain. This can lead to unnecessary anxiety or even inappropriate surgical procedures.
Furthermore, MRI scans are significantly more expensive and have much longer waiting times than standard X-rays. For the majority of people, the results of an MRI will not change the first-line management of the condition, which focuses on exercise, muscle strengthening, and weight care. As established in the clinical guidance provided by the NHS, the focus should remain on your symptoms and function rather than just what a scan shows.
Investigating the causes of joint locking
If you experience a sensation where your joint becomes completely stuck or ‘locks’, this is a common trigger for an MRI. This mechanical issue is often caused by a loose body, a small piece of cartilage or bone, floating in the joint space. An MRI is the only non-invasive way to locate these fragments and determine if they need to be removed. Keeping the supporting muscles strong can often provide enough stability to minimise these sensations, but a formal scan helps determine if the internal architecture of the joint has been significantly disrupted.
Identifying triggers for a diagnostic scan
Clinical guidance from NICE emphasises that the decision to use advanced imaging should be based on specific red flags. If you notice a sudden increase in joint heat, redness, or if your pain feels ‘electrical’ or sharp regardless of activity, these are triggers for a more detailed review. For most individuals, however, staying active and following a structured management plan is more effective than waiting for an MRI that may only confirm what is already known through a physical exam.
Differentiation: Structural wear vs Acute injury
It is essential to differentiate between the structural wear of osteoarthritis and acute soft tissue injuries that require different care. Osteoarthritis develops slowly over time and is characterised by activity-related pain and short-lived morning stiffness. In contrast, an acute injury, such as a torn ACL or a sudden meniscal tear, usually follows a specific event and causes immediate, intense swelling and instability. An MRI is the gold standard for identifying these acute issues, but for the gradual changes of osteoarthritis, the clinical assessment of a general practitioner remains the most important diagnostic tool.
Conclusion
MRI scans are highly useful for identifying soft tissue injuries, loose fragments, and early inflammation, but they are rarely necessary for the routine diagnosis of osteoarthritis. While they provide a detailed view of the joint’s internal environment, a clinical diagnosis based on symptoms and a physical exam is often sufficient to begin an effective management plan. In many cases, the high sensitivity of an MRI can lead to findings that are not actually responsible for the pain, highlighting why healthcare professionals prioritise your function and daily symptoms over imaging alone. By focusing on strengthening the supporting muscles and staying mobile, you can manage the condition effectively without the need for advanced scans in the early stages.
If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why did my doctor order an X-ray instead of an MRI?
An X-ray is excellent for seeing bone spurs and joint space narrowing, which are the main markers of osteoarthritis, and it is a quicker and more accessible first step.
Can an MRI see cartilage better than an X-ray?
Yes. Cartilage is invisible on an X-ray but appears clearly on an MRI, allowing for a direct assessment of its thickness and surface health.
Does an MRI show if I need surgery?
An MRI can help a surgeon see the state of the soft tissues, but the decision for surgery is usually based on your level of pain and how much the condition affects your daily life.
Is it normal for an MRI to show a tear I didn’t know I had?
Yes. Many minor meniscal tears are a normal part of ageing and do not cause symptoms, which is why an MRI result must be carefully matched to your physical pain.
Should I request an MRI if my joint is clicking?
Clicking is very common in osteoarthritis and is usually not a reason for an MRI unless the joint is also locking or catching painfully.
How long does an MRI take compared to an X-ray?
An MRI usually takes thirty to sixty minutes and requires you to remain still, while an X-ray takes only a few minutes.
Authority Snapshot
This article was written by Dr. Stefan Petrov, a UK-trained physician with an MBBS and postgraduate certifications including Basic Life Support (BLS), Advanced Cardiac Life Support (ACLS), and the UK Medical Licensing Assessment (PLAB 1 & 2). He has hands-on experience in general medicine, surgery, anaesthesia, ophthalmology, and emergency care. Dr. Petrov has worked in both hospital wards and intensive care units, performing diagnostic and therapeutic procedures, and has contributed to medical education by creating patient-focused health content and teaching clinical skills to junior doctors.
