Do people with coeliac disease have higher risk of bone thinning?
In the UK, it is well-established that coeliac disease significantly increases the risk of bone thinning, including both osteopenia and osteoporosis. Coeliac disease is an autoimmune condition where the immune system reacts to gluten by damaging the lining of the small intestine. This damage directly interferes with the body’s ability to absorb the essential nutrients required for skeletal strength. According to the NHS, many people are only diagnosed with coeliac disease after they have suffered an unexpected fragility fracture or after a DEXA scan reveals low bone mineral density.
What We’ll Discuss in This Article
- How intestinal damage leads to nutrient malabsorption
- The critical link between coeliac disease and Vitamin D deficiency
- Why a gluten-free diet is the first step in protecting your bones
- UK clinical guidelines: When to request a DEXA scan for coeliac disease
- Secondary factors: Inflammation and hormonal changes
- Managing your long-term bone health after a coeliac diagnosis
Malabsorption: The root of bone thinning in coeliac disease.
The primary reason coeliac disease affects the bones is the damage to the ‘villi’, the tiny, finger-like projections that line the small intestine and absorb nutrients from food.
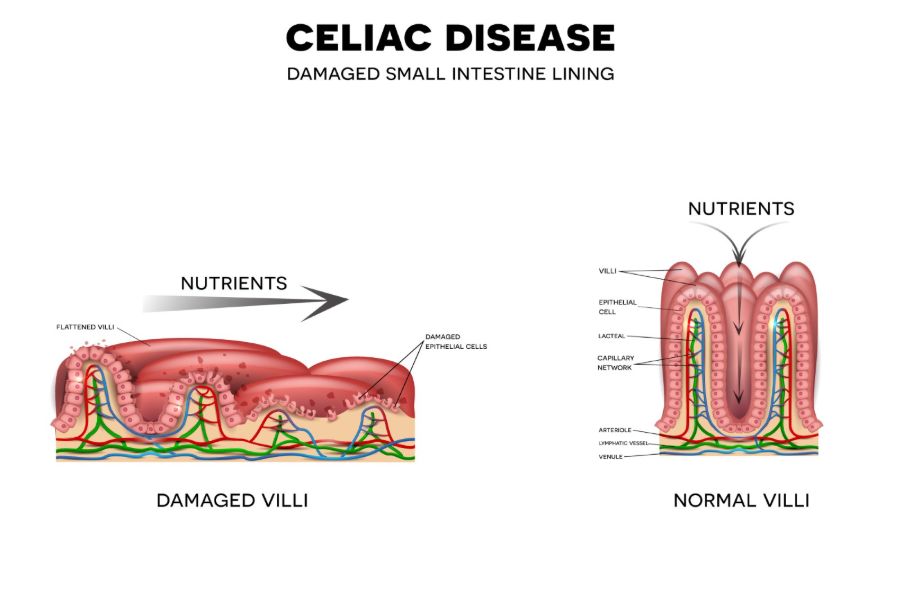
When a person with coeliac disease eats gluten, these villi become inflamed and flattened. This results in malabsorption, where the body cannot take in enough:
- Calcium: The primary building block of bone mineral.
- Vitamin D: The “key” that allows the gut to absorb calcium into the bloodstream.
- Magnesium and Vitamin K: Secondary but vital nutrients for the bone matrix.
Even if you have a diet rich in these nutrients, the damaged intestine simply cannot process them, leading the body to “leach” calcium from the bones to maintain steady levels in the blood.
Chronic inflammation and “Secondary Hyperparathyroidism.”
Beyond malabsorption, the autoimmune nature of coeliac disease creates a “pro-inflammatory” environment in the body. Inflammatory markers can directly stimulate osteoclasts, the cells that dissolve bone.
Furthermore, if the body senses a constant lack of calcium in the blood due to malabsorption, it triggers the parathyroid glands to release more hormone (PTH). This is known as Secondary Hyperparathyroidism. High levels of PTH tell the body to break down bone tissue even faster to release calcium into the circulation, rapidly accelerating the thinning process.
UK clinical monitoring for coeliac patients.
Because the risk is so high, the National Institute for Health and Care Excellence (NICE) provides specific recommendations for bone health in coeliac disease.
- DEXA Scan at Diagnosis: Adults diagnosed with coeliac disease are often referred for a bone density scan at the time of diagnosis, especially if they have other risk factors or were diagnosed later in life.
- Regular Blood Tests: Your GP or gastroenterologist will regularly check your calcium, vitamin D, and “bone profile” to ensure you are not becoming deficient.
- Repeat Scans: If bone thinning is detected, scans are typically repeated every two to five years to monitor the effectiveness of treatment.
Can a gluten-free diet reverse bone loss?
The good news is that once you adopt a strict, lifelong gluten-free diet, the intestinal villi usually begin to heal. This allows your body to start absorbing bone-healthy nutrients properly again.
For many people in the UK, bone density can improve significantly within the first year or two of starting a gluten-free diet. However, if the damage was severe or if the diagnosis was delayed, the bones may not return to “normal” density on their own, and additional bone-strengthening medication (like bisphosphonates) may be required.
Conclusion
People with coeliac disease are at a much higher risk of bone thinning due to the direct impact of malabsorption and systemic inflammation. In the UK, bone health is considered a core part of coeliac disease management. The most effective way to protect your skeleton is through strict adherence to a gluten-free diet, supplemented by adequate calcium and vitamin D as prescribed by your medical team. By catching bone thinning early through a DEXA scan, you can take steps to prevent future fractures and maintain an active lifestyle. If you are concerned about your bone strength or have recently been diagnosed with coeliac disease, seek a medical review. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Do I need a DEXA scan if I was diagnosed with coeliac disease as a child?
If your coeliac disease was well-managed from childhood, your risk is lower, but a baseline scan in early adulthood is still often recommended to ensure you reached your “Peak Bone Mass.”
Should I take extra calcium “just in case”?
You should aim for at least 1,000mg of calcium a day. However, always talk to your GP before starting high-dose supplements, as they will need to check your current blood levels first.
Does “silent” coeliac disease (no stomach symptoms) still affect bones?
Yes, even if you don’t have obvious digestive issues, the immune response can still damage the villi and lead to “silent” bone loss.
Are gluten-free substitute foods good for bones?
Many gluten-free flours and breads in the UK are fortified with calcium and iron to help replace what is lost through malabsorption. Check the labels for “fortified” status.
Can I get my vitamin D from sunlight alone if I have coeliac disease?
In the UK, sunlight is only sufficient from April to September. For someone with coeliac disease, a year-round supplement is often safer to guarantee adequate levels.
Why does my doctor check my parathyroid (PTH) levels?
High PTH is a signal that your body is struggling to get enough calcium from your diet and is instead taking it from your bones.
Is it safe to exercise if I have coeliac-related osteoporosis?
Yes, weight-bearing exercise is essential to help “signal” your bones to strengthen, but you should consult a physiotherapist for a plan that is safe for your specific density levels.
Authority Snapshot (E-E-A-T Block)
This article examines the clinical intersection of autoimmune gastrointestinal health and bone mineral density within the UK healthcare framework. It has been written and reviewed by Dr. Stefan Petrov, a UK-trained physician, to ensure the information is accurate and reflects current NHS and NICE standards. The content is designed to help patients manage the long-term skeletal implications of coeliac disease.
