Are women more likely to develop RA or PsA?
Inflammatory arthritis encompasses several conditions that cause the immune system to attack the joints, but these conditions do not affect all groups of people in the same way. Statistical evidence in the United Kingdom shows clear differences in how Rheumatoid Arthritis and Psoriatic Arthritis manifest across different sexes. Understanding these patterns of prevalence is essential for public health awareness and helps individuals recognise when their specific risk profile might be higher due to biological or environmental factors.
What We’ll Discuss in This Article
- The higher prevalence of Rheumatoid Arthritis in women
- Why Psoriatic Arthritis affects men and women at similar rates
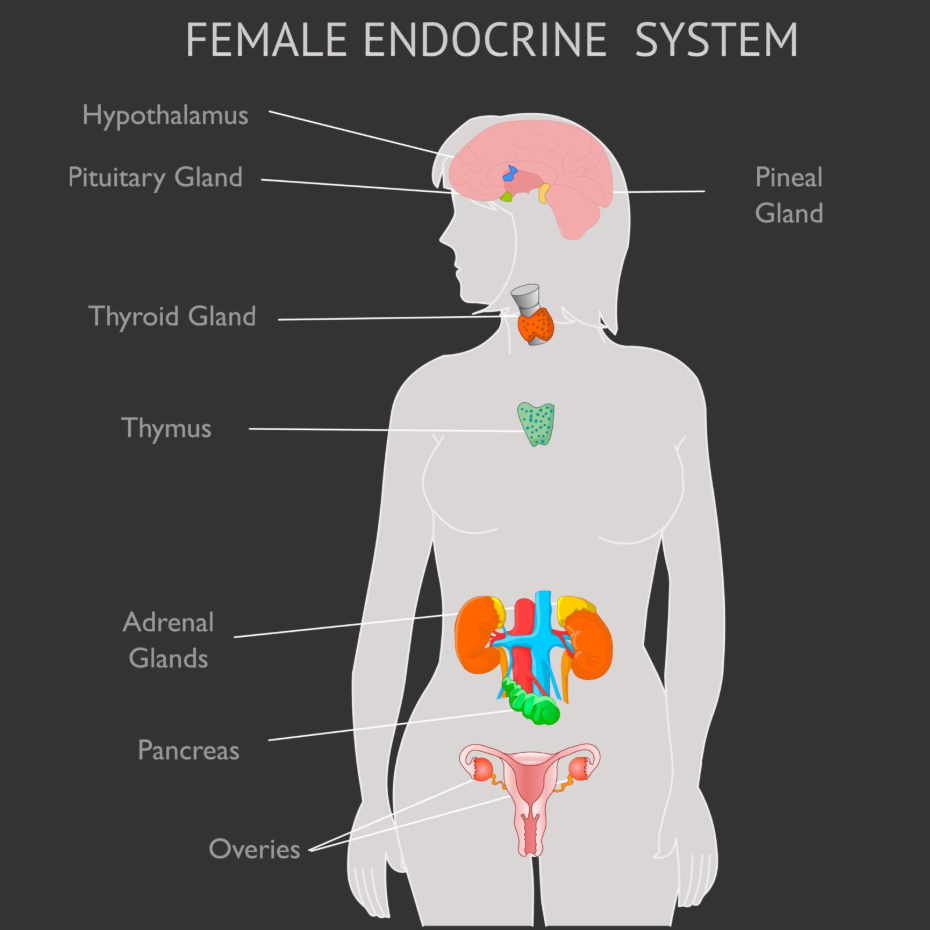
- The influence of hormones and the endocrine system on joint health
- Common ages of onset for different sexes in inflammatory conditions
- Biological and genetic factors that contribute to autoimmune risk
- Patterns of symptom severity across different demographics
- When to seek urgent medical attention for inflammatory symptoms
Women are significantly more likely to develop Rheumatoid Arthritis (RA) than men, with some estimates suggesting they are diagnosed two to three times as often. Conversely, Psoriatic Arthritis (PsA) tends to affect men and women roughly equally, showing no major sex bias in general prevalence. These differences are often attributed to a complex interplay of sex hormones, genetic predispositions, and the way the female immune system is naturally structured to respond to internal and external triggers.
Sex Prevalence in Rheumatoid Arthritis
Rheumatoid Arthritis is one of the most common autoimmune conditions in the UK, and it shows a very distinct sex-based pattern. According to the NHS, rheumatoid arthritis is more common in women than in men. While it can develop at any age, women are typically diagnosed between the ages of 30 and 50, whereas men are often diagnosed later in life. The reasons for this higher incidence in females are not fully understood, but researchers point towards the role of oestrogen and other reproductive hormones in stimulating the immune response.
Beyond just the frequency of diagnosis, the way the disease progresses can also differ. Women with RA sometimes report more widespread joint involvement and higher levels of fatigue compared to men. However, men who develop the condition may be at a slightly higher risk of experiencing extra-articular complications, such as lung involvement or cardiovascular issues. This disparity highlights the importance of personalised monitoring, as the condition can behave differently depending on the patient’s biological sex.
Sex Prevalence in Psoriatic Arthritis
Unlike Rheumatoid Arthritis, Psoriatic Arthritis does not show a strong preference for one sex over the other. The NHS states that psoriatic arthritis affects men and women equally. This condition is closely linked to the skin condition psoriasis, and because psoriasis itself affects both sexes at similar rates, the associated joint inflammation follows a similar equalised pattern. Most people develop PsA between the ages of 30 and 50, although it can occur at any time.
While the overall numbers are equal, there are subtle differences in how the condition presents in men versus women. Some clinical observations suggest that men are more likely to experience axial involvement, which is inflammation focused on the spine and sacroiliac joints. Women, on the other hand, may be more likely to experience polyarthritis, where many small joints like those in the fingers and toes are affected simultaneously. Despite these variations in presentation, the diagnostic process and treatment goals remain largely the same for both groups.
Comparison of RA and PsA Prevalence
The following table provides a comparison of how these two conditions typically affect different sexes within the UK population.
| Feature | Rheumatoid Arthritis (RA) | Psoriatic Arthritis (PsA) |
| Sex Prevalence | Significantly more common in women | Affects men and women equally |
| Typical Ratio (W:M) | Approximately 3:1 | Approximately 1:1 |
| Peak Age of Onset | 30 to 50 years (earlier in women) | 30 to 50 years |
| Symmetry of Symptoms | Usually symmetrical (both sides) | Often asymmetrical |
| Common Initial Site | Small joints of hands and feet | Large joints or fingers/toes |
The Role of Hormones in Inflammatory Arthritis
The high rate of autoimmune conditions in women is frequently linked to the endocrine system. Oestrogen, the primary female sex hormone, is known to interact with the immune system by modulating the activity of white blood cells. This can make the immune system more reactive, which is beneficial for fighting infections but can increase the risk of the system mistakenly attacking healthy tissue. Many women notice that their arthritis symptoms fluctuate during times of significant hormonal change, such as during the menstrual cycle, pregnancy, or menopause.
Pregnancy often provides a temporary period of relief for women with RA, as the body naturally suppresses certain parts of the immune system to protect the foetus. However, it is very common for a significant flare-up to occur shortly after childbirth when hormone levels shift rapidly. Similarly, the onset of menopause is a peak time for RA diagnosis, suggesting that the decline in oestrogen levels may play a role in “switching on” the condition in those who are genetically predisposed.
Genetic and Environmental Influences
While sex and hormones are major factors, they do not act in isolation. Genetics play a foundational role in determining who will develop inflammatory arthritis. Certain genetic markers, such as the HLA-DRB1 gene in RA or the HLA-B27 gene in PsA, can be passed down through families. While these genes are found in both men and women, the way they interact with sex hormones may explain why women are more likely to reach the threshold for clinical disease in certain types of arthritis.
Environmental factors also contribute to these prevalence rates. Smoking is a major risk factor for RA and is known to be particularly damaging for those with a genetic predisposition. Historically, higher smoking rates in men may have narrowed the gap in prevalence, but as smoking habits have changed, the biological predominance in women has become more apparent. Occupational exposures and physical joint trauma can also act as triggers, with joint injuries sometimes being the catalyst for Psoriatic Arthritis following a skin flare.
Conclusion
Women are much more likely to develop Rheumatoid Arthritis than men, while Psoriatic Arthritis affects both sexes at approximately equal rates. These differences are largely driven by hormonal influences and genetic factors that govern how the immune system responds to internal triggers. Recognising these patterns helps in understanding individual risk and ensures that symptoms are not dismissed when they align with known demographic trends. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can men still develop severe Rheumatoid Arthritis?
Yes, while it is less common in men, those who do develop RA can experience severe symptoms and may be more prone to complications affecting the lungs and heart.
Does Psoriatic Arthritis always start after the skin condition?
In most cases, the skin condition psoriasis appears first, but around one in five people will experience joint pain and swelling before any skin patches are noticed.
Why does menopause affect arthritis risk?
The significant drop in oestrogen during menopause can alter immune regulation and may trigger the onset of inflammatory symptoms in women who are already susceptible.
Are there specific types of arthritis that are more common in men?
Gout and ankylosing spondylitis are two examples of inflammatory conditions that traditionally show a higher prevalence in men than in women.
Is Juvenile Idiopathic Arthritis more common in girls?
Some subtypes of JIA are more common in girls, particularly oligoarthritis, which often affects young children and focuses on a small number of joints.
Does hormone replacement therapy (HRT) help with RA?
The relationship between HRT and RA is complex and should be discussed with a specialist, as it may help some symptoms while having little effect on others.
Can a father pass the risk of PsA to his daughter?
Yes, the genetic markers for Psoriatic Arthritis can be inherited from either parent and can affect children of any sex.
Authority Snapshot (E-E-A-T Block)
This article was produced to provide clear and evidence-based information on the sex-based prevalence of inflammatory arthritis in the UK. The content is authored by the Medical Content Team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine and emergency care. All information presented is strictly aligned with NHS and NICE clinical guidance to ensure public safety and accuracy.
