

The heart relies on a steady, coordinated electrical signal to pump blood efficiently throughout the body. When these signals become chaotic, the result is an arrhythmia, with Atrial Fibrillation (AF) being the most common type encountered in the UK. AF is often described by patients as a ‘fluttering’ or ‘thumping’ sensation, but its implications go far beyond simple discomfort. Because it affects how blood moves through the heart, it carries specific risks that other arrhythmias may not. Understanding what makes AF unique and how it compares to other heart rhythm problems is essential for anyone monitoring their cardiovascular health. This article provides a clear, medically neutral guide to AF and its clinical significance.
What We’ll Discuss in This Article
- The clinical definition of Atrial Fibrillation and how it affects the heart’s chambers.
- Common symptoms of AF, including palpitations, fatigue, and breathlessness.
- A comparison of AF against other arrhythmias like SVT and Atrial Flutter.
- Why AF is considered a major risk factor for stroke and heart failure.
- The biological causes and lifestyle triggers that initiate an AF episode.
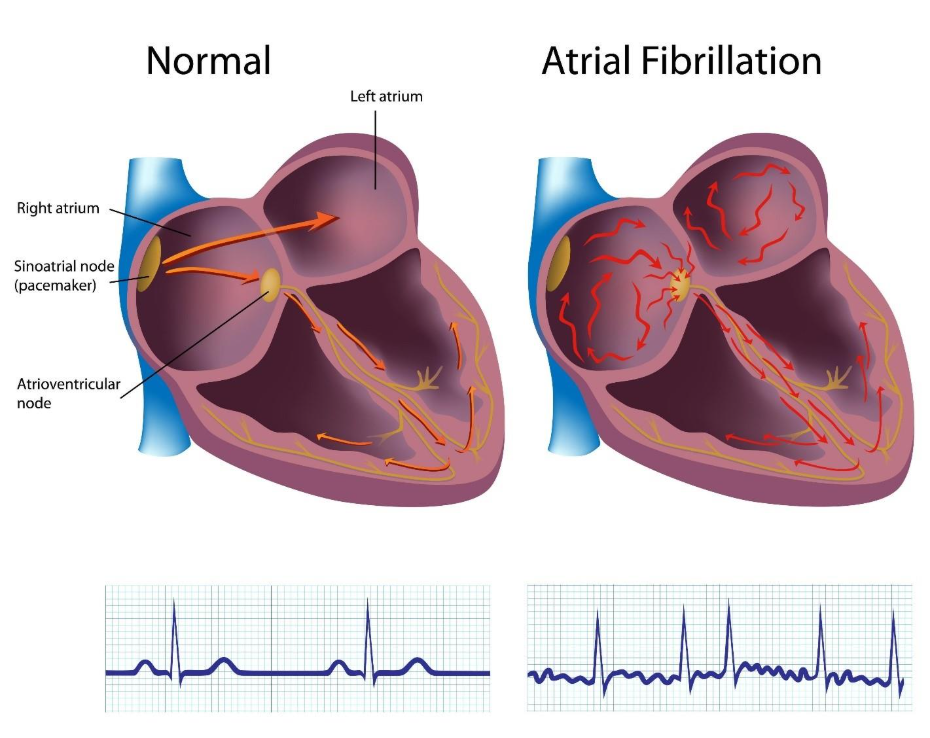
- How clinicians differentiate AF from other heart rhythm issues using an ECG.
- Emergency safety guidance for sudden or severe cardiac symptoms.
What is Atrial Fibrillation (AF)?
Atrial Fibrillation (AF) is a heart rhythm disorder where the upper chambers of the heart (atria) beat chaotically and out of sync with the lower chambers (ventricles). This results in an irregular and often abnormally fast heart rate, which can lead to poor blood flow. According to NHS guidance, while a normal heart rate is between 60 and 100 beats per minute, in AF, the heart rate can be considerably higher.
Expanded Explanation
In a healthy heart, a single electrical impulse travels a precise path to cause a contraction. In AF, multiple electrical signals fire randomly from different parts of the atria, causing them to quiver (fibrillate) rather than squeeze.
- The Atrial ‘Quiver’: Instead of a powerful contraction, the atria twitch rapidly, sometimes up to 400 times per minute.
- Irregular Pulse: Because the gateway to the lower chambers (the AV node) cannot let all these signals through, it sends them down randomly, creating the ‘irregularly irregular’ pulse characteristic of AF.
- Types of AF: AF can be paroxysmal (it comes and goes), persistent (lasts more than seven days), or permanent.
Clinical Context
AF is the most common sustained arrhythmia in the UK, affecting roughly 1 in 45 people. It is often discovered during routine pulse checks or when a patient presents with unexplained tiredness. Because it can be ‘silent’, meaning it causes no symptoms, it is a leading focus of UK public health initiatives to prevent secondary complications.
How Serious is AF Compared with Other Arrhythmias?
AF is considered highly serious because it is a leading cause of preventable stroke and heart failure, making it clinically distinct from many ‘benign’ arrhythmias. While some rhythm issues like ectopic beats are harmless flutters, AF increases the risk of stroke by up to five times. According to NICE guidance, AF is responsible for approximately 20 per cent of all strokes in the UK, which are often more severe than strokes from other causes.
Seriousness vs. Other Arrhythmias
- AF vs. SVT: Supraventricular Tachycardia (SVT) is often distressing but rarely leads to blood clots. AF is more serious because the quivering atria allow blood to pool, which is the primary cause of stroke-related clots.
- AF vs. Ectopic Beats: Ectopic beats are isolated ‘extra’ beats that do not usually affect the heart’s long-term health. AF is a sustained rhythm change that can weaken the heart muscle over time.
- AF vs. Ventricular Arrhythmias: Rhythms starting in the lower chambers (ventricles) are often more immediately life-threatening. However, AF is more common and carries a higher long-term risk of chronic disability from stroke or heart failure.
Impact on Cardiac Function
If the heart remains in AF for long periods, the constant fast and irregular beating can cause the heart muscle to tire and stretch. This leads to tachycardia-induced cardiomyopathy, a form of heart failure where the heart becomes too weak to pump enough blood for the body’s needs.
Causes of Atrial Fibrillation
AF is usually caused by structural or electrical changes in the heart tissue, often as a result of other long-term health conditions that put the heart under pressure.
- High Blood Pressure: This is the most common cause, as hypertension forces the heart to work harder, eventually causing the atria to enlarge and their electrical pathways to become unstable.
- Coronary Artery Disease: Narrowed arteries can reduce the blood supply to the heart’s electrical system, causing it to malfunction.
- Heart Valve Disease: Leaky or narrowed valves can cause blood to back up into the atria, stretching the tissue and triggering chaotic signals.
- Overactive Thyroid: Excessive thyroid hormone acts as a powerful stimulant to the heart muscle and is a frequent cause of new-onset AF.
- Ageing: The heart’s internal wiring naturally undergoes fibrous changes as we get older, which is why AF is much more common in those over the age of 65.
Triggers for AF Episodes
For individuals with paroxysmal AF, certain external factors can ‘spark’ an episode, causing the heart to suddenly slip into an irregular rhythm.
- Alcohol Consumption: Binge drinking is a well-known trigger, often referred to as ‘holiday heart syndrome’ in UK clinical practice.
- Caffeine and Stimulants: High amounts of caffeine from energy drinks or coffee can irritate the atria and trigger an episode in sensitive individuals.
- Physical and Emotional Stress: Major surgery, severe infections (like pneumonia), or intense emotional shock can cause surges in adrenaline that disrupt the heart rhythm.
- Dehydration and Electrolyte Shift: A lack of fluids or low levels of potassium and magnesium can make the heart’s electrical nodes more irritable.
- Sleep Apnoea: Dips in oxygen levels during sleep put significant strain on the atria, making it a major risk factor and trigger for AF.
Differentiation: AF vs. Atrial Flutter vs. SVT
It is important to distinguish AF from other fast rhythms, as the treatment paths and stroke risks vary significantly.
| Feature | Atrial Fibrillation (AF) | Atrial Flutter | SVT |
| Pulse Quality | Completely irregular. | Often regular but very fast. | Usually very regular and fast. |
| Electrical Pattern | Chaotic quivering. | Organised ‘sawtooth’ waves. | Regular fast loops. |
| Stroke Risk | High; requires anticoagulation. | High; similar to AF. | Generally low. |
| Typical Sensation | Fluttering or shuffling. | Racing or pounding. | Sudden, intense racing. |
| Primary Risk | Stroke and Heart Failure. | Stroke and Heart Failure. | Fainting or Distress. |
Conclusion
Atrial Fibrillation (AF) is an irregular heart rhythm that is uniquely serious due to its direct link to stroke and heart failure. While many people experience palpitations from harmless causes, the quivering motion of the atria in AF allows blood to pool and clot, making it a high-priority clinical condition. By identifying the causes and avoiding known triggers like alcohol and stress, individuals can manage the frequency of their episodes. Most importantly, early diagnosis through pulse checks and ECGs allows for the use of effective treatments, such as blood thinners and rate-control medications, which significantly reduce the risk of life-altering complications.
If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can AF go away without treatment?
Paroxysmal AF comes and goes on its own, but the underlying tendency usually remains and may require management to prevent it from becoming permanent.
Is AF always a medical emergency?
Not usually, provided you feel stable; however, it becomes an emergency if you have chest pain, feel like you will faint, or have signs of a stroke.
Can I have a stroke if my AF doesn’t cause symptoms?
Yes, ‘silent’ AF carries the same stroke risk as symptomatic AF, which is why regular pulse checks are recommended for high-risk groups.
Why is AF more common as we get older?
Natural wear and tear on the heart’s electrical system, combined with years of managing blood pressure, makes the atria more prone to rhythm issues.
Does everyone with AF need blood thinners?
Not everyone; clinicians use a scoring system (CHA2DS2-VASc) to determine your individual stroke risk before prescribing anticoagulants.
Can exercise trigger Atrial Fibrillation?
While moderate exercise is healthy, extremely intense endurance sports can occasionally act as a trigger for some individuals.
What is the ‘FAST’ test in relation to AF?
The FAST test helps recognise a stroke, which is a complication of AF: Face fallen, Arms cannot be raised, Speech slurred, Time to call 999.
Authority Snapshot (E-E-A-T Block)
This article was written by Dr. Rebecca Fernandez, a UK-trained physician with an MBBS and extensive clinical experience across cardiology, emergency medicine, and internal medicine. In this guide, we will define Atrial Fibrillation (AF), explore its physical impact, and compare its clinical seriousness to other common heart rhythm disorders. This information follows NHS and NICE standards to provide a safe, accurate, and reassuring overview of heart health.
