What heart rhythm problems require an ICD?
An Implantable Cardioverter Defibrillator (ICD) is a sophisticated electronic device designed to protect individuals from life threatening heart rhythms. Unlike a standard pacemaker, which primarily manages a slow heart rate, an ICD is capable of detecting and stopping dangerously fast rhythms that can lead to sudden cardiac arrest. In the UK, these devices are essential for patients with specific electrical or structural heart conditions.
In this article, you will learn about the primary heart rhythm disorders that necessitate an ICD, such as ventricular tachycardia and ventricular fibrillation. We will also explore the underlying causes of these disturbances, the triggers that can lead to an acute event, and how an ICD differs from other cardiac devices. Finally, we will cover the clinical standards used by the NHS to identify who is most at risk.
What We’ll Discuss in This Article
- Key heart rhythm problems including ventricular tachycardia and fibrillation
- The role of an ICD in preventing sudden cardiac arrest
- Underlying causes like cardiomyopathy and previous heart attacks
- Common triggers for dangerous heart rhythm episodes
- The difference between an ICD and a standard pacemaker
- Diagnostic criteria used by UK heart teams
- Essential emergency guidance for cardiac symptoms
What are the main heart rhythm problems that require an ICD?
An ICD is required for heart rhythm problems that originate in the lower chambers of the heart, known as the ventricles. The most common issues are ventricular tachycardia (VT) and ventricular fibrillation (VF). These rhythms are dangerous because they are too fast for the heart to pump blood effectively to the brain and body. An ICD monitors these rhythms and delivers an electrical shock to reset the heart if a lethal rhythm occurs.
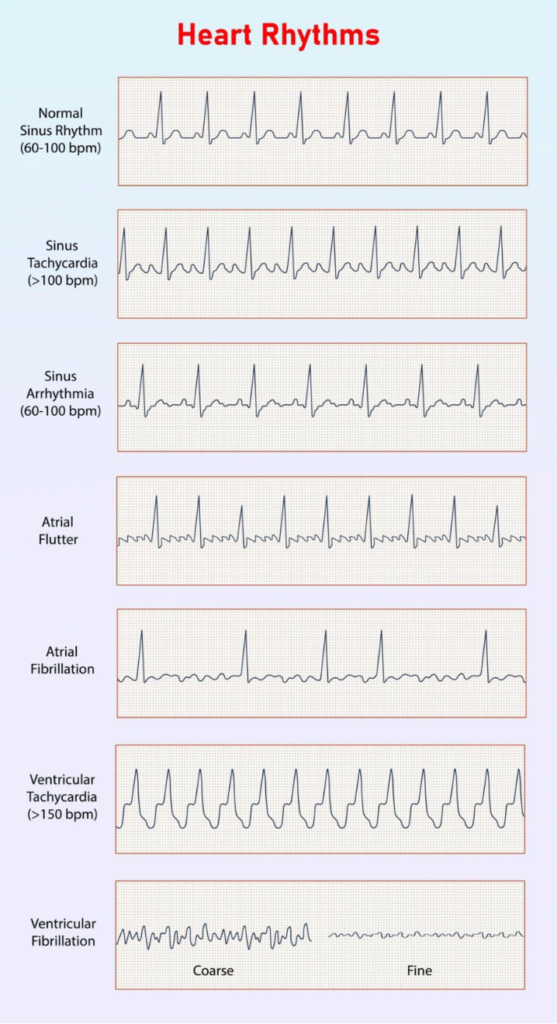
Ventricular tachycardia involves a heart rate that is significantly faster than normal, usually over 100 beats per minute, which can cause dizziness or fainting. Ventricular fibrillation is even more severe; it involves chaotic, rapid electrical activity that causes the heart to quiver instead of pumping. Without immediate intervention, VF leads to a total loss of consciousness and cardiac arrest. An ICD is the only way to provide an immediate internal solution for these conditions.
- Ventricular Tachycardia (VT): A fast, regular rhythm that can be stable or unstable.
- Ventricular Fibrillation (VF): A chaotic, irregular rhythm that is always a medical emergency.
- Sustained Arrhythmias: Rhythms that last long enough to cause a drop in blood pressure.
- Inherited Syndromes: Specific genetic conditions that predispose individuals to these fast rhythms.
Identifying candidates for ICD implantation
Candidates for an ICD are typically divided into two groups: primary prevention and secondary prevention. Primary prevention refers to patients who have not yet had a dangerous rhythm but are at high risk, often due to significant heart muscle weakness. Secondary prevention refers to patients who have already survived a cardiac arrest or a life threatening episode of ventricular tachycardia.
NICE guidelines in the UK use specific measures, such as the ejection fraction, to identify candidates. The ejection fraction is a percentage that represents how much blood is pumped out of the heart with each beat. If this number is below a certain threshold, typically 35%, the risk of a dangerous rhythm increases, making an ICD a standard recommendation even if the patient feels well.
- Primary Prevention: For those with a weakened heart muscle and a high risk of future events.
- Secondary Prevention: For survivors of a previous life threatening arrhythmia or cardiac arrest.
- Low Ejection Fraction: A key clinical measure of heart pump function used in the UK.
- Symptomatic Patients: Individuals who experience blackouts or severe palpitations.
Causes of dangerous heart rhythms
The need for an ICD is often the result of structural changes to the heart muscle that disrupt the normal flow of electricity. In the UK, the most frequent cause is ischaemic heart disease, where a previous heart attack has left behind a patch of scar tissue. This scar tissue cannot conduct electricity, forcing the heart’s natural signals to take detour routes that can loop back on themselves and trigger a fast rhythm.
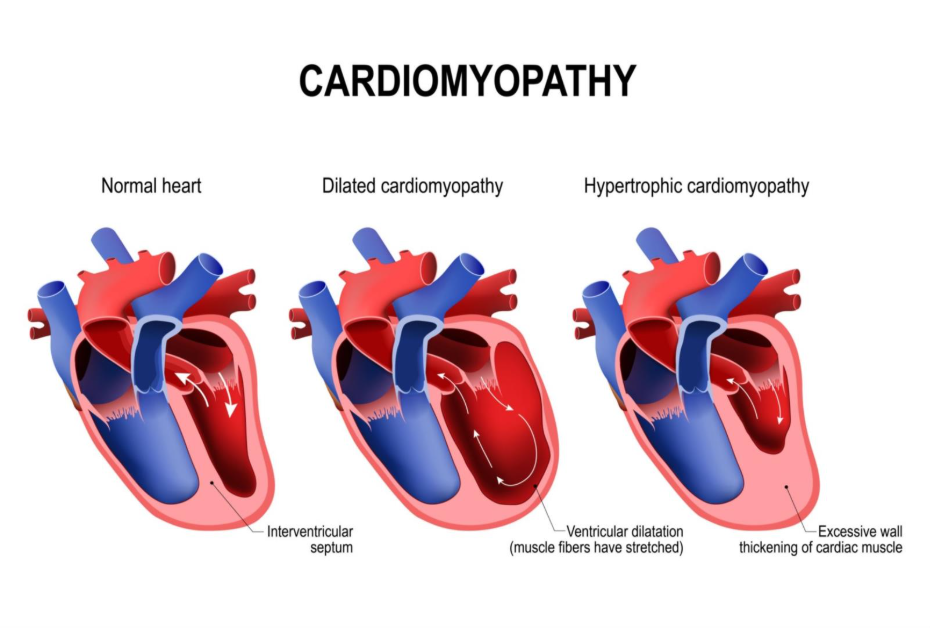
Other common causes include various types of cardiomyopathy, which is a disease of the heart muscle. Hypertrophic cardiomyopathy causes the heart walls to become abnormally thick, while dilated cardiomyopathy causes the heart to become enlarged and thin. Both conditions can create the perfect environment for electrical instability. Additionally, inherited genetic conditions like Long QT Syndrome or Brugada Syndrome can cause dangerous rhythms even in a heart that appears structurally normal on a scan.
- Previous Heart Attack: Scar tissue provides a foundation for short circuiting electrical paths.
- Dilated Cardiomyopathy: A weakened, enlarged heart muscle that stretches electrical pathways.
- Hypertrophic Cardiomyopathy: Thickened heart muscle that can obstruct flow and disrupt signals.
- Genetic Conditions: Inherited ion channel disorders that affect the heart’s electrical recovery.
Triggers for acute arrhythmic events
While the underlying cause of a heart rhythm problem is often chronic, certain triggers can cause a dangerous episode to occur suddenly. In a heart that is already vulnerable, a sudden spike in adrenaline can be enough to set off an episode of ventricular tachycardia. This is why some patients are advised to avoid extreme physical exertion or intense emotional stress until their device is fitted.
Other triggers include severe electrolyte imbalances, particularly low levels of potassium or magnesium in the blood. These minerals are essential for the stable electrical function of heart cells. Acute illnesses, such as severe pneumonia or a new heart attack, can also put the heart under enough strain to trigger a lethal rhythm. Certain medications, including some antibiotics or antidepressants, can also lengthen the heart’s electrical cycle and act as a trigger in susceptible individuals.
- Physical Exertion: Sudden, intense activity that spikes heart rate and adrenaline.
- Electrolyte Imbalance: Low potassium or magnesium levels disrupting cellular stability.
- Acute Infection: Systemic stress that increases the workload of a weakened heart.
- Medication Interactions: Specific drugs that can prolong the heart’s electrical intervals.
Differentiation: ICD vs. Pacemaker
It is important to understand that an ICD and a pacemaker are not the same thing, although they look similar. A pacemaker is a low energy device designed to treat a heart that beats too slowly. It monitors the rhythm and sends a tiny electrical pulse only when the heart misses a beat. Most people cannot feel their pacemaker working because the energy used is so low.
An ICD is a more powerful device designed to treat a heart that beats too fast. While most modern ICDs have a pacemaker function built in, their defining feature is the ability to deliver a high energy shock. This shock is intended to stop the chaotic rhythm and allow the heart’s natural pace to restart. This is often described as a single ‘kick in the chest’ and is a life saving intervention rather than a subtle rhythmic support.
Conclusion
An ICD is a vital intervention for patients in the UK who are at risk of life threatening heart rhythms like ventricular tachycardia or fibrillation. Whether used as a safety net for a weakened heart or as a protection for survivors of cardiac arrest, the device provides an immediate response to electrical emergencies. By understanding the conditions and triggers associated with these rhythms, patients can manage their heart health more effectively alongside their clinical team.
If you experience severe, sudden, or worsening symptoms, such as crushing chest pain, a sudden blackout, or severe shortness of breath, call 999 immediately.
Is an ICD bigger than a pacemaker?
Yes, an ICD is typically larger because it requires a bigger battery and a capacitor to store the energy needed for a shock.
Can an ICD battery be replaced?
The entire generator is replaced during a simple procedure when the battery runs low, which usually happens every 5 to 9 years.
Will I always get a shock if my heart goes fast?
No, many ICDs are programmed to try ‘anti tachycardia pacing’ first, which is a series of fast, small pulses to bring the heart back to normal without a shock.
Can I drive with an ICD in the UK?
There are strict DVLA rules regarding driving; you must inform the DVLA, and you may be unable to drive for a period depending on why the device was fitted.
Is it safe to have an MRI with an ICD?
Many modern ICDs are MRI conditional, but you must inform the clinical team so the device can be placed in a special mode during the scan.
What happens if I get a shock while I am alone?
You should sit or lie down immediately and follow the plan provided by your hospital, which usually involves contacting your ICD clinic or calling 999.
Does an ICD prevent heart attacks?
No, an ICD treats the electrical rhythm but does not prevent the blockages in the arteries that cause a heart attack.
Authority Snapshot
This article was written by Dr. Rebecca Fernandez, a UK trained physician with an MBBS and extensive experience in cardiology, intensive care, and emergency medicine. Dr. Fernandez has managed critically ill patients and stabilised acute cardiac cases, providing her with deep insight into the life saving role of cardiac devices. This content follows the latest NHS and NICE guidelines to ensure accurate and evidence based information for the public.
