Can conditions like atrial fibrillation or heart failure occur alongside coronary artery disease?
When you are diagnosed with Coronary Artery Disease (CAD), it is overwhelming enough. Hearing that you also have ‘Heart Failure’ or ‘Atrial Fibrillation’ can feel like a devastating blow. However, these conditions are not random, unrelated bad luck. They are often intimately linked parts of the same story. Think of the heart as a house: if the pipes (arteries) are blocked, the water pressure drops (heart failure), and the electrical wiring (rhythm) can short-circuit. It is very common to have two, or even all three, of these conditions at once.
What We’ll Discuss in This Article
- The ‘Domino Effect’: How blocked arteries can trigger pump failure and rhythm issues.
- Heart Failure: Why a ‘starved’ heart muscle eventually becomes a weak one.
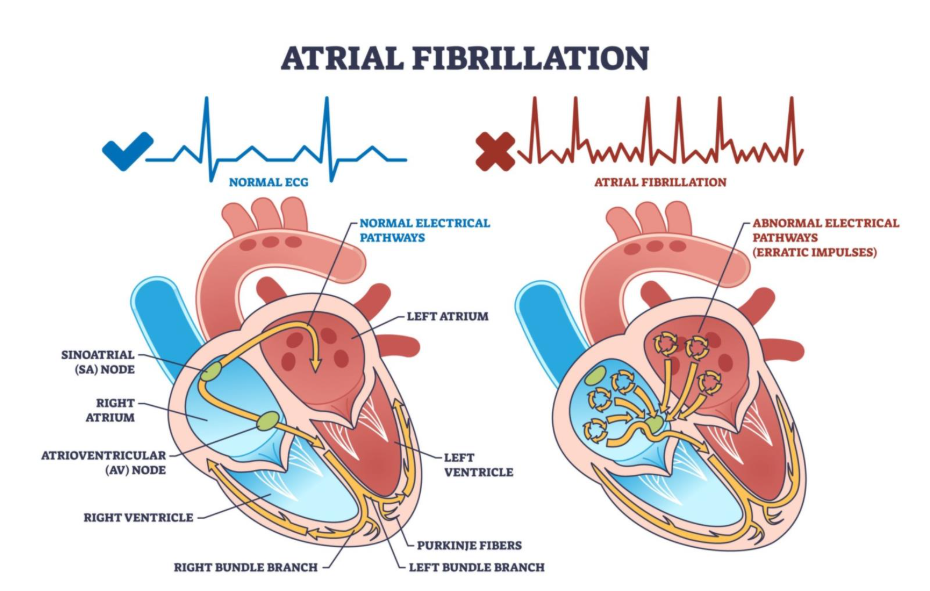
- Atrial Fibrillation (AFib): The electrical chaos caused by heart stress.
- The ‘Triple Threat’ Treatment: How one medication (like beta-blockers) can treat all three.
- Blood Thinner Balance: The delicate mix of Aspirin vs. Anticoagulants.
- Prognosis: Why having more than one condition is manageable, not hopeless.
The Connection: Coronary Artery Disease as the Root Cause
CAD is often the first domino to fall.
Coronary Artery Disease means the fuel pipes supplying the heart muscle are narrowed.
- The Pump (Heart Failure): If the muscle is constantly starved of oxygen (ischemia), or if a heart attack kills a patch of muscle, the heart becomes too weak or stiff to pump blood effectively. This is called Ischaemic Cardiomyopathy. In fact, CAD is the single most common cause of heart failure.
- The Rhythm (AFib): When the heart is struggling to pump against blocked arteries or high blood pressure, the upper chambers (atria) stretch. This stretching damages the electrical pathways, causing the chaotic rhythm known as Atrial Fibrillation.
Heart Failure: It Doesn’t Mean the Heart ‘Stops’
The term ‘Heart Failure’ is frightening, but misleading. It means ‘Heart Inefficiency.’
If you have CAD and Heart Failure, it usually means your heart is pumping at a reduced capacity (e.g., 35% instead of 60%).
- The Symptoms: You might feel breathless when lying flat, have swollen ankles, or feel exhausted after minor effort.
- The Good News: Fixing the arteries (with stents or bypass surgery) can often restore blood flow to the ‘hibernating’ muscle, causing the heart function to improve significantly.
Atrial Fibrillation: The Stroke Risk
AFib is an electrical problem, but its biggest risk is a clot.
If you have CAD, your blood is already prone to clotting on the rough plaque. If you add AFib, the chaotic heartbeat causes blood to pool and clot in the heart itself.
- The Danger: If a clot travels from the heart to the brain, it causes a stroke. According to the British Heart Foundation, having Atrial Fibrillation increases your risk of stroke by five times compared to someone with a normal rhythm.
- The Management: This requires careful medication management (see below) to thin the blood without causing bleeding.
Managing the ‘Triple Threat’ (The Overlap)
Doctors love ‘Two-for-One’ medications.
Because these conditions are so linked, the treatments overlap beautifully. You likely won’t need three separate bags of pills.
- Beta-Blockers (e.g., Bisoprolol): The MVP drug. It slows the heart (helping AFib), reduces oxygen demand (helping Angina), and protects the muscle (helping Heart Failure).
- ACE Inhibitors (e.g., Ramipril): These relax arteries to lower blood pressure (helping Angina) and prevent the heart from enlarging (helping Heart Failure).
The Blood Thinner Challenge
This is the only tricky part.
- For CAD (Stents): We use Antiplatelets (like Aspirin or Clopidogrel) to stop platelets sticking to the metal stent.
- For AFib: We use Anticoagulants (like Apixaban or Warfarin) to stop blood pooling in the atria.7
- The Conflict: Taking both together (‘Triple Therapy’) massively increases bleeding risk.
- The Solution: Your cardiologist will carefully balance this. Usually, you take the antiplatelet for a short time (e.g., 6–12 months after a stent) and then drop it, staying on just the anticoagulant for life.
Conclusion
Having CAD alongside Heart Failure or AFib does not mean you are ‘worse off’ than someone with just one; it just means your heart needs a more comprehensive maintenance plan. The interventions for one (like fixing the arteries) often dramatically improve the others (improving the pump). Modern cardiology is designed to treat the heart as a whole system, not just a collection of broken parts.
Would you like me to create a ‘Symptom Checker’ table that helps you distinguish between Angina pain, AFib palpitations, and Heart Failure breathlessness?
Can a pacemaker fix this?
If you have Heart Failure and specific electrical delays (LBBB), a special pacemaker called CRT (Cardiac Resynchronisation Therapy) can force the heart to pump more efficiently. Standard pacemakers don’t fix the blocked arteries, but they stop the heart beating too slowly.
Is it safe to exercise with all three?
Yes, but you must start slow. Cardiac Rehabilitation is even more important for you. Exercise strengthens the muscles, meaning the heart doesn’t have to work as hard to pump blood to them.
Will I need open heart surgery?
Not necessarily. Many patients are managed with medication and stents. However, if you have severe CAD and diabetes or heart failure, a bypass (CABG) is often the safest long-term option to restore fuel to the muscle.
Can AFib go away if I fix the arteries?
Sometimes. If the AFib was caused by acute ischemia (lack of oxygen), restoring blood flow can help the rhythm stabilize. However, often the electrical damage is permanent, and you will simply stay on medication to control it.
Why do I feel dizzy?
You are likely on medications that lower blood pressure and slow the heart rate. If you stand up too quickly, the blood drops to your feet. Take your time getting up, and tell your doctor if you actually faint.
Authority Snapshot
This article was written by Dr. Rebecca Fernandez, a UK-trained physician (MBBS) with extensive experience in acute medicine and cardiology. Dr. Fernandez frequently manages ‘multimorbidity’, patients who don’t just have one heart problem, but a combination. She explains how the heart’s ‘plumbing’ (arteries), ‘pump’ (muscle), and ‘electrics’ (rhythm) are all connected, helping you understand why these conditions often arrive together and how they are treated as a whole.
