What is the difference between COPD, chronic bronchitis and emphysema?
Chronic obstructive pulmonary disease ‘COPD’ is an umbrella term for a group of progressive lung conditions, of which chronic bronchitis and emphysema are the two most common types. The main difference lies in the area of the lung affected: chronic bronchitis involves long-term inflammation and excess mucus in the bronchial tubes ‘the airways’, while emphysema involves the permanent destruction of the air sacs ‘alveoli’ where oxygen enters the blood. Most people with a COPD diagnosis have a combination of both conditions.
What We will cover in this Article
- The clinical relationship between COPD, bronchitis, and emphysema.
- The physical impact of chronic bronchitis on the airway lining.
- How emphysema destroys the structural integrity of the air sacs.
- Distinctive symptoms used to differentiate the two phenotypes.
- How medical professionals diagnose the dominant condition.
- Modern management strategies for combined respiratory issues.
Defining the COPD Umbrella
COPD is not a single disease but a category of illnesses that cause persistent airflow blockage. It is a long-term condition that makes it difficult to breathe because the lungs have become damaged or inflamed. When a doctor uses the term COPD, they are typically referring to the combined effects of airway narrowing and tissue destruction.
In the UK, it is rare for a person to have only emphysema or only chronic bronchitis; usually, one condition is more prominent, but elements of both are present. This is why the broad term COPD is preferred in clinical settings to describe the overall impact on a patient’s respiratory health.
Chronic Bronchitis: The Airway Condition
Chronic bronchitis is defined as a productive cough that lasts for at least three months of the year for two consecutive years. It primarily affects the bronchial tubes, which carry air to the lungs.
When these tubes are constantly irritated, most commonly by tobacco smoke, they become inflamed and the lining thickens. This narrowing of the tubes, combined with an overproduction of thick mucus, makes it very difficult for air to pass through. This often leads to a persistent, phlegmy cough and a higher risk of frequent chest infections.
| Feature | Chronic Bronchitis Details |
| Primary Site | Bronchial tubes ‘Airways’ |
| Main Symptom | Frequent, productive ‘wet’ cough |
| Physical Change | Inflammation, swelling, and excess mucus |
| Common Indicator | Cyanosis ‘bluish tint’ and swelling in legs |
Emphysema: The Air Sac Condition
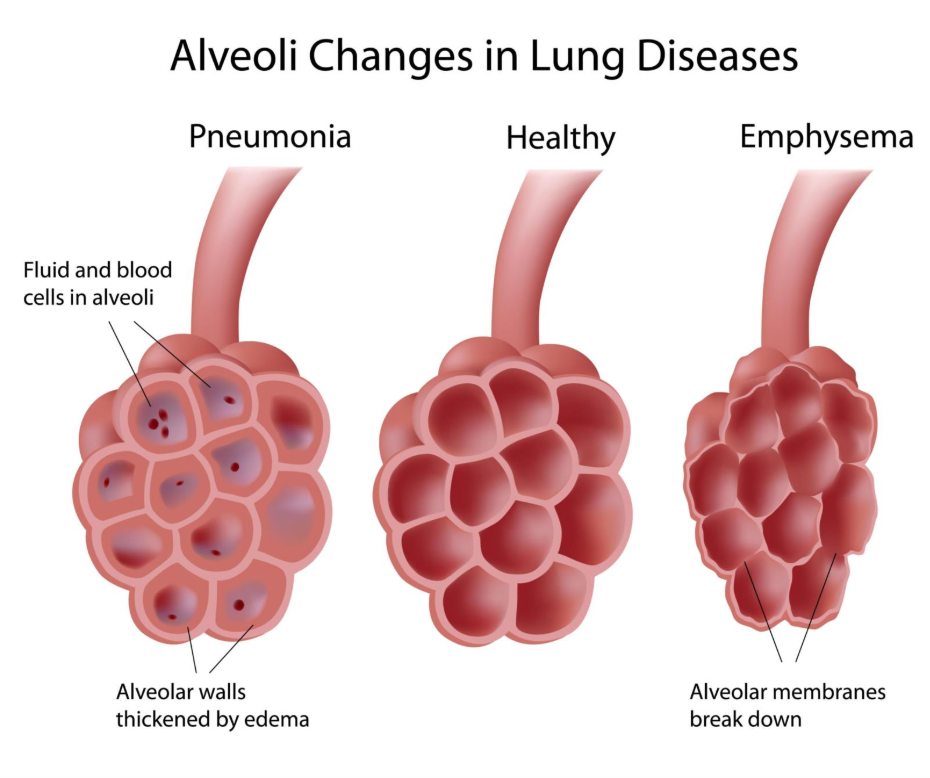
Emphysema affects the lungs at a deeper level, specifically in the alveoli. These are tiny, balloon-like sacs where the exchange of oxygen and carbon dioxide takes place. In a healthy lung, these sacs are elastic and springy.
In emphysema, the walls between these air sacs are destroyed, causing them to rupture and create larger, less efficient air pockets. Because the lungs lose their elasticity, they cannot deflate properly, and air becomes trapped. This leads to a sensation of constant breathlessness and can cause the chest to expand into a rounded ‘barrel’ shape.
Shutterstock
| Feature | Emphysema Details |
| Primary Site | Alveoli ‘Air Sacs’ |
| Main Symptom | Severe shortness of breath ‘Dyspnoea’ |
| Physical Change | Destruction of air sac walls and air trapping |
| Common Indicator | Weight loss and a ‘barrel-shaped’ chest |
Key Differences at a Glance
While both conditions lead to breathlessness and fall under the COPD label, their physical presentation and the way they affect daily life can vary significantly.
| Comparison Point | Chronic Bronchitis | Emphysema |
| Cough | Frequent and produces thick mucus. | Minimal or dry cough. |
| Breathlessness | Moderate, often worse during infections. | Severe and progressive. |
| Body Type | Patients may appear heavier or swollen. | Patients are often thin due to effort of breathing. |
| Oxygen Levels | Likely to experience lower oxygen early on. | Oxygen levels may stay stable until late stages. |
| Chest Appearance | Generally normal structure. | Often develops a ‘barrel chest’. |
To Summarise
The difference between COPD, chronic bronchitis, and emphysema is essentially the difference between a category and its specific components. COPD is the over-arching diagnosis, while chronic bronchitis describes the inflamed, mucus-filled airways and emphysema describes the destroyed, inelastic air sacs. Understanding which condition is dominant helps medical teams tailor treatments to improve breathing and overall quality of life.
If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can you have COPD without having emphysema?
Yes, it is possible to have COPD that is almost entirely driven by chronic obstructive bronchitis with very little destruction of the air sacs.
Why is it important to distinguish between the two?
Identifying the dominant phenotype helps in choosing the right medications; for example, some treatments are better at clearing mucus, while others focus on keeping air sacs from collapsing.
Is emphysema worse than chronic bronchitis?
Neither is inherently ‘worse’, but emphysema involves the permanent destruction of lung tissue, whereas the inflammation in bronchitis can sometimes be slightly more responsive to medication.
Do the treatments differ significantly?
While both use bronchodilator inhalers, those with dominant chronic bronchitis may require more help with mucus clearance, whereas those with severe emphysema may be candidates for lung volume reduction procedures. (Uploader: please link this to the article on ‘Surgical options for COPD’).
Authority Snapshot
This article provides a clinical comparison of respiratory conditions based on UK medical standards and common patient presentations.
- Reviewer: Dr. Stefan Petrov. Dr. Petrov is a UK-trained physician with an MBBS and postgraduate certifications in BLS and ACLS. He has hands-on experience in general medicine, surgery, and emergency care. He has worked in intensive care units and hospital wards, focusing on diagnostic and therapeutic procedures.
- Clinical Standards: This content is written to reflect the 2026 understanding of COPD phenotypes and management protocols.
- Integrity Note: This information is for general educational purposes and does not replace a professional clinical diagnosis or lung function assessment.
