Why is smoking the main risk factor for COPD and emphysema?
Smoking is the primary cause of Chronic Obstructive Pulmonary Disease and emphysema because it introduces a high concentration of toxins and oxidants directly into the lungs. These substances trigger a relentless inflammatory response that destroys the structural integrity of the air sacs and narrows the bronchial tubes over time.
What we will discuss in this article
- The chemical impact of tobacco smoke on lung tissue
- How smoking paralyses, the lungs’ natural cleaning system
- The destruction of elastin and its role in emphysema
- Statistical data on smokers and lung function decline
- Why even occasional smoking contributes to long term damage
The chemical assault on the airways
Every puff of tobacco smoke contains thousands of chemicals, including nicotine, tar, and carbon monoxide. These chemicals act as irritants that cause the lining of the airways to swell and produce excess mucus. In a healthy person, mucus is cleared by tiny hairs called cilia. However, smoking paralyses and eventually kills these cilia, meaning the irritants and mucus stay trapped in the lungs.
- Oxidative Stress: Smoke contains free radicals that directly damage cell membranes.
- Inflammatory Cell Recruitment: The body sends white blood cells to the lungs to fight the irritants, but these cells release enzymes that unintentionally break down lung tissue.
- Mucus Hypersecretion: Chronic irritation leads to the permanent enlargement of mucus producing glands.
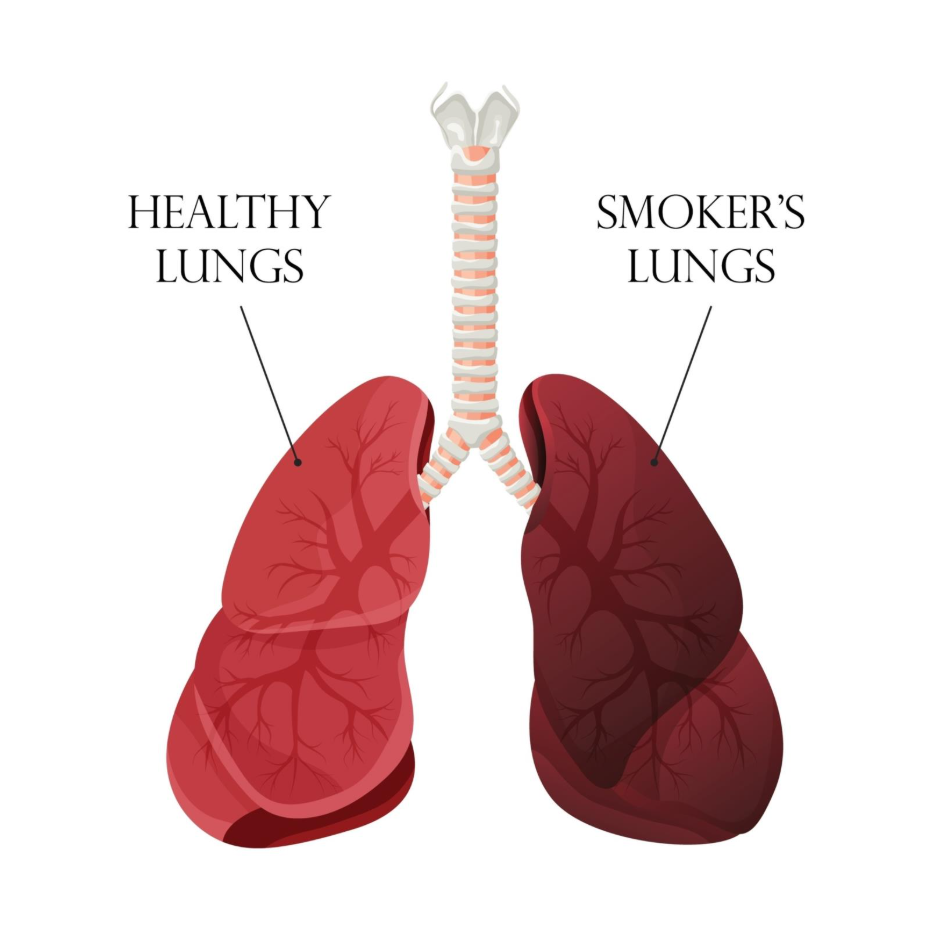
Destruction of the air sacs
Emphysema is specifically characterised by the destruction of the alveoli or air sacs. Tobacco smoke inhibits a protein called alpha 1 antitrypsin, which normally protects the lungs. Without this protection, enzymes produced by the immune system eat away at the elastin in the alveolar walls. Once this elastin is gone, the air sacs lose their springiness and eventually rupture.
| Component of Smoke | Effect on Lung Function | Resulting Condition |
| Tar | Clogs cilia and coats lung tissue | Chronic Bronchitis |
| Oxidants | Destroys alveolar wall elasticity | Emphysema |
| Nitrogen Oxides | Causes airway constriction | Airflow Obstruction |
| Carbon Monoxide | Reduces oxygen carrying capacity | Systemic Fatigue |
Lung function and smoking data
Clinical data shows that while everyone loses some lung function as they age, smokers lose it at a significantly accelerated rate. This is often measured using FEV1, which is the amount of air a person can exhale in one second.
- Non smokers: Typically lose about 25 to 30 millilitres of lung function per year after age 25.
- Susceptible Smokers: Can lose 80 to 100 millilitres per year.
- Cumulative Damage: The risk of developing COPD is directly proportional to ‘pack years’ or the total amount smoked over a lifetime.
Summary
Smoking is the main risk factor because it causes a triple threat of damage: it paralyses the lungs’ cleaning mechanism, triggers chronic inflammation, and destroys the elastic tissue required for breathing. This combination leads to the permanent airway narrowing and air sac destruction that defines COPD and emphysema. Protecting the lungs from tobacco smoke is the most effective way to prevent these debilitating conditions.
If you experience severe sudden or worsening symptoms call 999 immediately.
How long does it take for smoking to cause COPD?
It usually takes decades of exposure. Most people are diagnosed after age 40, though the damage begins with the very first cigarette.
Does switching to light cigarettes reduce the risk?
No. Light or menthol cigarettes do not reduce the risk of COPD, as the same toxic chemicals are still inhaled into the lungs.
Why do some smokers not get COPD?
Genetics play a role. Some people have more resilient lung tissue, but even those who do not develop COPD will still suffer some level of lung damage and reduced function.
Authority snapshot
This article was prepared by our Medical Content Team and reviewed by Dr. Stefan Petrov to ensure clinical accuracy. It explains the pathophysiological link between tobacco use and obstructive lung disease according to established respiratory science. Our goal is to provide factual information to help individuals understand the risks of smoking.
