


Whether a brain tumour can be fully removed depends on its biological type, its location relative to critical neurological structures, and its degree of infiltration into healthy brain tissue. In the United Kingdom, neurosurgical teams prioritise the preservation of the patient’s quality of life, which often necessitates a balance between removing the maximum amount of abnormal growth and protecting vital functional areas. While some benign tumours with clear boundaries can be entirely excised, others may require a sub-total removal followed by supplementary treatments like radiotherapy or chemotherapy. Every surgical plan is developed through an integrated multidisciplinary review within the NHS to ensure that the approach is evidence-based and personalised to the individual’s needs. Understanding the complexities of surgical resection is essential for patients and families as they navigate the clinical pathways provided by the UK healthcare system. This article explores the different levels of surgical removal, the impact of tumour grade, and the advanced technologies used to enhance surgical precision.
What We’ll Discuss in This Article
- The distinction between gross total resection and sub-total removal.
- How the anatomical location of the tumour influences surgical feasibility.
- The impact of tumour grade and infiltrative growth on complete excision.
- Advanced technologies used in the UK to improve surgical accuracy.
- The role of adjuvant therapies when a tumour cannot be fully removed.
- Integrated post-operative monitoring and the role of the multidisciplinary team.
Gross Total Resection versus Sub-Total Removal
The term “gross total resection” is used when a surgeon is able to remove all visible parts of a brain tumour during an operation, as confirmed by post-operative imaging. Conversely, a “sub-total removal” or “debulking” occurs when only a portion of the mass is removed because the remaining tissue is too close to vital structures. The NHS states that the goal of surgery is to remove as much of the brain tumour as possible without damaging the surrounding healthy tissue.
Achieving a gross total resection is more common in tumours that are encapsulated or have distinct margins, such as many meningiomas. However, even when a scan shows no visible tumour remaining, microscopic cells may still exist at the margins. In the United Kingdom, surgeons use high-resolution intraoperative microscopes to aid this process. If a tumour is intertwined with critical blood vessels or nerves, the surgeon may intentionally leave a small “sliver” behind to prevent permanent neurological deficits. This clinical decision prioritises the patient’s functional independence over the absolute removal of every visible cell, reflecting a patient-centred approach to neurosurgery.
Impact of Anatomical Location on Removal
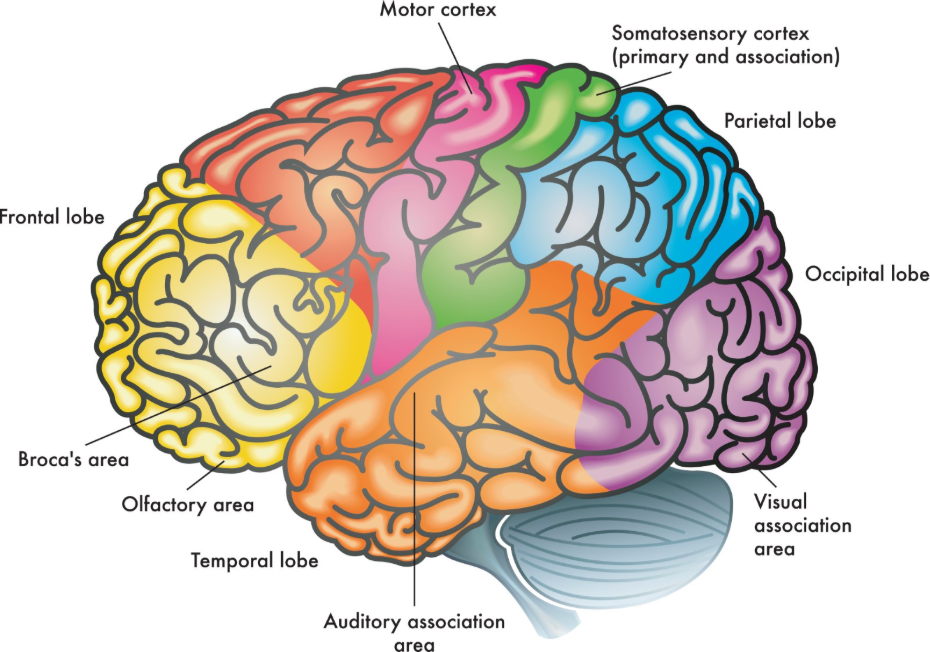
The anatomical location of a brain tumour is a primary factor in determining if a full removal is safely achievable, especially if the mass is situated in an “eloquent” area. Eloquent areas are those parts of the brain responsible for critical functions such as speech, motor control, or vision. NICE clinical guidelines for brain tumours indicate that for tumours located in eloquent areas, the risk of neurological deficit must be carefully balanced against the benefits of total removal.
| Location Category | Surgical Feasibility | Impact on Removal |
| Superficial Lobe | Generally accessible. | Higher likelihood of gross total resection. |
| Deep-seated / Midline | Difficult to reach. | Often requires sub-total removal or biopsy. |
| Brainstem | Extremely high risk. | Typically limited to biopsy or conservative care. |
| Eloquent Areas | Risk to speech/motor. | Removal limited by functional boundaries. |
Tumours located deep within the brain or near the brainstem present significant challenges because the surgical path required to reach them could damage essential healthy tissue. In such cases, the UK multidisciplinary team may recommend a sub-total removal to relieve pressure (debulking) rather than attempting a complete excision. This strategy aims to improve the patient’s symptoms while relying on non-surgical treatments to manage the remaining tumour. By assessing the anatomical “real estate” involved, UK neurosurgeons can provide a realistic surgical goal that protects the patient’s long-term health.
Infiltrative Growth and Tumour Grade
The biological grade and the growth pattern of a tumour significantly influence whether it can be fully removed, with high-grade tumours often being more difficult to excise completely. High-grade tumours, such as glioblastomas, are characterised by “infiltrative” growth, meaning they send root-like microscopic extensions into the healthy brain tissue well beyond the visible edges seen on a scan.
Because there is no clear border between the tumour and the healthy brain, a truly “full” removal at a microscopic level is often impossible for these types of growths. Low-grade tumours, while slower-growing, can also be infiltrative, although some benign variants remain self-contained. In the United Kingdom, pathologists provide detailed reports on the tumour’s characteristics to help the surgical team understand its behaviour. For infiltrative tumours, surgery is viewed as the first step in a combined management plan, intended to reduce the “tumour burden” so that subsequent therapies like radiotherapy can be more effective.
Technology to Enhance Surgical Precision
Neurosurgical centres in the United Kingdom utilise various advanced technologies to help surgeons identify the boundaries of a tumour and maximise the extent of removal safely. Neuronavigation acts like a GPS for the brain, using pre-operative scans to guide the surgeon’s instruments in real-time. The GOV.UK health pages provide clinical profiles indicating that intraoperative monitoring and mapping are standard tools used in the UK to improve the safety of tumour resection.
Technological aids used in the NHS include:
- Fluorescence-Guided Surgery: Using a dye (5-ALA) that makes malignant cells glow under a special light.
- Intraoperative Ultrasound: Providing real-time images during surgery to check for residual tumour.
- Electrophysiological Monitoring: Tracking nerve signals to ensure vital pathways are not disturbed.
- Awake Craniotomy: Allowing the patient to speak or move during surgery to protect eloquent areas.
These tools allow surgeons to be more precise, especially when distinguishing between abnormal tissue and healthy brain that looks identical to the naked eye. While technology cannot guarantee a 100% removal in every case, it significantly increases the “maximal safe resection” achieved in UK operating theatres. This integration of technology and expertise is a cornerstone of neurosurgical safety within the NHS.
Adjuvant Therapy for Residual Tumour
When a brain tumour cannot be fully removed due to its location or infiltrative nature, the clinical team implements “adjuvant” therapies to manage the remaining cells. These treatments are designed to target microscopic disease or any visible fragments that were left behind to protect neurological function.
Common adjuvant treatments in the UK include:
- Radiotherapy: Using targeted radiation beams to destroy remaining cells.
- Chemotherapy: Systemic medication to interfere with the growth of abnormal cells.
- Targeted Therapy: Drugs that attack specific molecular markers within the tumour.
- Active Surveillance: Regular scans for slow-growing residual tissue that does not require immediate treatment.
The multidisciplinary team coordinates the timing of these treatments to ensure they begin as soon as the surgical wound has healed. In the UK, this integrated approach recognises that surgery is often one part of a wider management framework. By combining surgical debulking with oncology, clinicians can manage the condition over the long term, even if a total physical removal was not achievable.
Integrated Monitoring and the MDT Role
Following surgery, every patient in the United Kingdom is monitored through an integrated pathway involving regular MRI scans and specialist consultations. The multidisciplinary team (MDT) reviews these scans to assess the baseline after surgery and to detect any signs of regrowth as early as possible.
The UK follow-up pathway ensures:
- Baseline Imaging: A scan performed shortly after surgery to confirm the extent of removal.
- Consistent Surveillance: Scheduled MRI scans to monitor any residual tumour.
- Specialist Review: Ongoing assessment of neurological and physical health.
- Collaborative Planning: Adjusting management if the residual tumour shows signs of change.
This structured system provides a safety net for patients, ensuring that those with residual tumour tissue remain under close clinical oversight. In the UK, the MDT brings together specialists from multiple fields to ensure that the transition from surgery to long-term monitoring is seamless. By following these national standards, the NHS provides a consistent and high level of care for patients throughout their recovery and beyond.
Conclusion
Whether a brain tumour can be fully removed depends on a complex interplay between its anatomical location, its biological grade, and its relationship with critical brain functions. In the UK, the NHS prioritise “maximal safe resection,” using advanced technology to remove as much of the mass as possible while protecting the patient’s functional independence. While some benign tumours can be entirely excised, infiltrative or high-grade tumours often require a combined approach of surgery and adjuvant therapies like radiotherapy. The multidisciplinary team coordinates this integrated care pathway to ensure that management is safe, evidence-based, and tailored to the individual. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does a “full removal” mean the tumour will never come back?
Not necessarily; even after a gross total resection, microscopic cells can remain, which is why regular follow-up scans are essential in the UK.
What if the surgeon can only remove a small part of the tumour?
Removing even a portion (debulking) can relieve pressure and symptoms, making subsequent treatments like radiotherapy more effective.
Can a tumour be “inoperable”?
A tumour is considered inoperable if its location means surgery would cause unacceptable neurological damage; in these cases, other treatments are used.
Why do I need a scan after surgery if the surgeon said they got it all?
A post-operative scan provides a baseline to confirm the extent of removal and is a mandatory part of the UK clinical pathway.
Is a second operation possible if the tumour grows back?
Yes; in the UK, the multidisciplinary team will assess if a second surgery is safe and beneficial if a tumour recurs.
Does the size of the tumour affect how much can be removed?
Size is a factor, but the tumour’s location and whether it has clear borders are often more important in determining the success of the removal.
How soon after surgery will I know if it was all removed?
You will usually have a post-operative MRI scan within 48 to 72 hours, and the results will be discussed with you shortly after.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the removal of brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in general surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


