


A brain tumour can cause vision or hearing problems by physically pressing on the sensory nerves or by disrupting the specific areas of the brain responsible for processing sight and sound. Because the brain acts as the central hub for interpreting all sensory information, any structural growth within the skull can interfere with the delicate pathways that connect the eyes and ears to the central nervous system.The UK healthcare system utilise a structured diagnostic pathway, involving high-resolution imaging and specialist reviews, to determine if a mass is the underlying cause of such sensory disruptions. Understanding the relationship between brain health and the senses is essential for patients to recognise when to seek medical advice. By following evidence-based protocols established by the NHS and NICE, clinical teams aim to manage these symptoms while addressing the physical growth to protect the patient’s long-term functional independence.
What We’ll Discuss in This Article
- How tumours in the occipital and temporal lobes affect sensory processing.
- The impact of increased intracranial pressure on the optic nerve.
- Tumours affecting the cranial nerves, including acoustic neuromas.
- Distinguishing between primary sensory issues and neurological causes.
- Management strategies for vision and hearing changes in the UK.
- UK clinical pathways for the urgent assessment of sensory deficits.
Vision Problems and the Impact of Location
Vision problems occur when a brain tumour interferes with the visual pathways or the primary visual cortex, located in the occipital lobe at the back of the brain. The brain processes visual signals through a complex route starting at the eyes, passing through the optic nerves, and ending in the rear of the cerebrum. The NHS states that a brain tumour can cause symptoms by increasing the pressure inside the skull or by damaging the part of the brain where the tumour is growing.
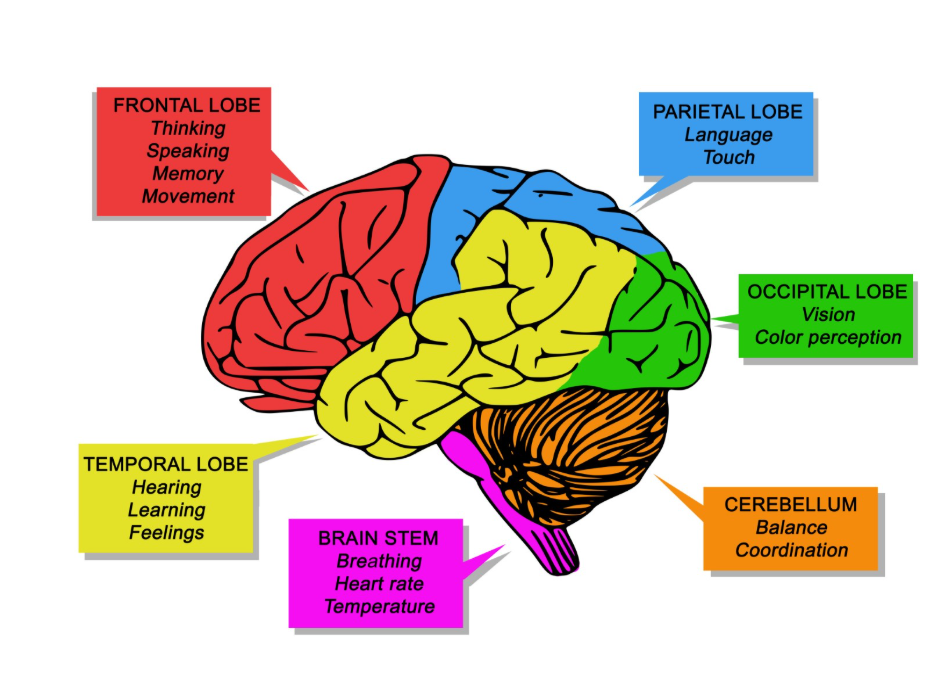
If a tumour grows in the occipital lobe, it can lead to vision loss, such as losing one side of the field of vision in both eyes (hemianopia). Growths in the temporal or parietal lobes can also affect the processing of visual information, leading to difficulties in recognising objects or perceiving movement. In the United Kingdom, clinicians assess these changes during a neurological examination by checking the patient’s peripheral vision and their ability to follow moving objects. Because these symptoms often develop gradually, they may first be noticed as a loss of coordination or an increase in minor accidents. Identifying these focal deficits helps UK medical teams pinpoint the area of the brain requiring urgent imaging.
Increased Intracranial Pressure and the Optic Nerve
A brain tumour can also cause vision problems indirectly by increasing the overall pressure within the skull, which can lead to swelling of the optic disc at the back of the eye. This condition, known as papilloedema, occurs when the high pressure interferes with the normal circulation of fluids around the optic nerve. NICE clinical guidelines for brain tumours indicate that any new-onset vision change associated with features of increased intracranial pressure should be reviewed by a specialist.

Symptoms of papilloedema include blurred vision, double vision (diplopia), or brief “blackouts” of vision, especially when bending over or coughing. In the UK, an optician may be the first to identify this swelling during a routine eye test, as it is visible as a blurring of the optic disc margins. Because the skull is a rigid container, even a slow-growing tumour can cause this pressure to rise over time. Managing this pressure is a clinical priority in the UK to prevent permanent damage to the optic nerve. Early detection through regular eye examinations and reporting visual changes to a GP are essential steps in the diagnostic process.
Hearing Problems and Acoustic Neuromas
Hearing problems can be caused by tumours that grow on the cranial nerves or in the parts of the brain responsible for interpreting sound. An acoustic neuroma, also known as a vestibular schwannoma, is a common non-cancerous tumour that grows on the nerve used for hearing and balance which leads from the inner ear to the brain.
These tumours typically cause a gradual loss of hearing in one ear, often accompanied by a ringing sound known as tinnitus. | The GOV.UK health pages provide clinical profiles for tumours affecting the cranial nerves, ensuring that specialist care is coordinated across the NHS. In the United Kingdom, patients with these symptoms are often referred to an Ear, Nose, and Throat (ENT) specialist for an initial hearing test before being referred for brain imaging. Identifying the specific nature of the hearing loss helps clinicians differentiate it from standard age-related changes or ear infections.
Distinguishing Sensory Origins and Neurological Causes
In the UK clinical setting, it is vital to distinguish between sensory problems originating in the eyes or ears themselves and those caused by a structural issue in the brain. Most vision problems are related to refractive errors or age-related eye conditions, while most hearing issues are caused by ear canal blockages or noise damage.
However, sensory changes caused by a brain tumour are often accompanied by other neurological “red flags,” such as persistent headaches, nausea, or changes in personality. A key indicator of a neurological cause is if the sensory loss is sudden, progressive, or involves both eyes or ears in an unusual pattern. For example, losing the same side of vision in both eyes is almost always a sign of a brain-based issue rather than an eye problem. Clinicians use a detailed history and physical examination to look for these patterns. While an eye or hearing test is a useful starting point, any persistent sensory symptom that does not improve with standard treatments requires a thorough investigation to rule out a mass within the skull.
Management of Sensory Symptoms in the UK
Management of vision and hearing problems associated with a brain tumour in the United Kingdom involves a multidisciplinary approach that targets the underlying growth while supporting the patient’s functional needs. Once a tumour is addressed through surgery, radiotherapy, or other methods, the focus often shifts to rehabilitative support to manage any remaining sensory deficits.
This can include working with ophthalmologists or audiologists who specialise in neurological recovery. For patients with permanent vision or hearing loss, the NHS provides access to sensory support services that offer advice on living with these changes and utilizing adaptive technologies. In some cases, reducing the pressure on the brain through medication can lead to a significant improvement in vision. For hearing issues related to cranial nerve tumours, management may focus on preserving the remaining hearing or managing tinnitus. This comprehensive care system ensures that the patient’s sensory health is prioritised alongside their physical recovery, fostering a holistic approach to neurological well-being.
UK Clinical Pathways for Sensory Assessment
The United Kingdom uses integrated care pathways to ensure that patients reporting persistent sensory changes are assessed thoroughly to identify any structural neurological causes. This typically begins with a GP review or an assessment by an optician or audiologist, followed by a specialist referral if a neurological cause is suspected.
The UK diagnostic pathway includes:
- Initial Assessment: Review of sensory history and any associated neurological “red flag” symptoms.
- Specialist Referral: Access to neurologists, neurosurgeons, or ENT specialists for advanced testing.
- Urgent Imaging: Fast-tracked MRI or CT scans to visualise the internal structures of the brain.
- MDT Discussion: A Multidisciplinary Team of experts determining the best management plan for the tumour and symptoms.
This structured system ensures that serious conditions are identified early, providing a clear route for those whose sensory shifts are related to a brain growth. By following these national protocols, the NHS provides a safety net that catches complex neurological issues while offering reassurance and support to the patient throughout their diagnostic and management journey.
Conclusion
A brain tumour can cause significant vision or hearing problems by disrupting the specific lobes responsible for sensory processing or by increasing pressure within the skull. These symptoms often manifest as blurred vision, one-sided hearing loss, or a reduction in the visual field and require professional clinical evaluation. In the UK, the NHS provides a clear pathway for investigating these changes to identify if a structural growth is the underlying cause. While many sensory issues are not serious, persistent or unusual changes should always be reported to a healthcare professional. Consistent monitoring and expert diagnosis are essential for protecting long-term neurological health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does a blurry eye always mean I have a brain tumour?
No; blurred vision is far more commonly caused by needing a new glasses prescription, dry eyes, or other common eye conditions.
Can an optician see a brain tumour?
An optician cannot see the tumour itself, but they can see swelling of the optic nerve (papilloedema), which is a sign of high pressure in the brain.
If my hearing loss is in both ears, is it likely a tumour?
Hearing loss in both ears is much more likely to be caused by age or noise exposure; tumours like acoustic neuromas typically affect only one ear.
Will my vision go back to normal after surgery?
Many patients see an improvement in vision once the pressure on the brain is relieved, though some may have permanent changes depending on the damage.
Can a brain tumour affect my sense of taste or smell?
Yes; tumours located near the olfactory or gustatory nerves can interfere with these senses, although this is less common than vision or hearing changes.
How long should I wait before seeing a doctor about vision changes?
In the UK, any sudden or persistent change in your vision should be reviewed by an optician or GP as soon as possible.
Is tinnitus a common sign of a brain tumour?
Tinnitus can be a symptom of an acoustic neuroma, but it is much more frequently caused by hearing loss or ear infections.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding brain tumours and sensory changes, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in emergency care, surgery, and clinical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


