


Diverticulitis can lead to serious medical complications such as a perforation or an abscess if the acute inflammation and infection of the diverticular pouches are not effectively managed. While most cases of diverticulitis are uncomplicated and resolve with conservative treatment, approximately one in five individuals may experience more severe issues that affect the integrity of the colon wall. A perforation occurs when a small tear develops in the weakened wall of a pouch, potentially allowing intestinal contents to leak into the abdominal cavity. An abscess is a localised collection of pus that forms as the body attempts to contain a bacterial infection near the site of the inflamed diverticula. In the United Kingdom, healthcare professionals categorise diverticulitis as either uncomplicated or complicated based on the presence of these findings, typically using diagnostic imaging to guide the clinical pathway. Understanding the biological progression from simple inflammation to a structural complication is vital for recognising the importance of timely medical intervention. By adhering to the evidence-based protocols established by the NHS and NICE, clinicians aim to resolve these complications while minimising the risk of long-term damage to the digestive tract. Proactive management and early detection of red-flag symptoms remain the primary strategies for maintaining bowel health during an acute flare-up.
What We’ll Discuss in This Article
- The biological mechanism behind the formation of diverticular abscesses.
- How a perforation develops and its impact on the abdominal cavity.
- The clinical relationship between localised infection and peritonitis.
- Diagnostic tools used in the UK to identify complicated diverticulitis.
- Potential long-term consequences such as fistulas or bowel obstructions.
- UK clinical pathways for managing severe diverticular complications.
The Formation and Management of Diverticular Abscesses
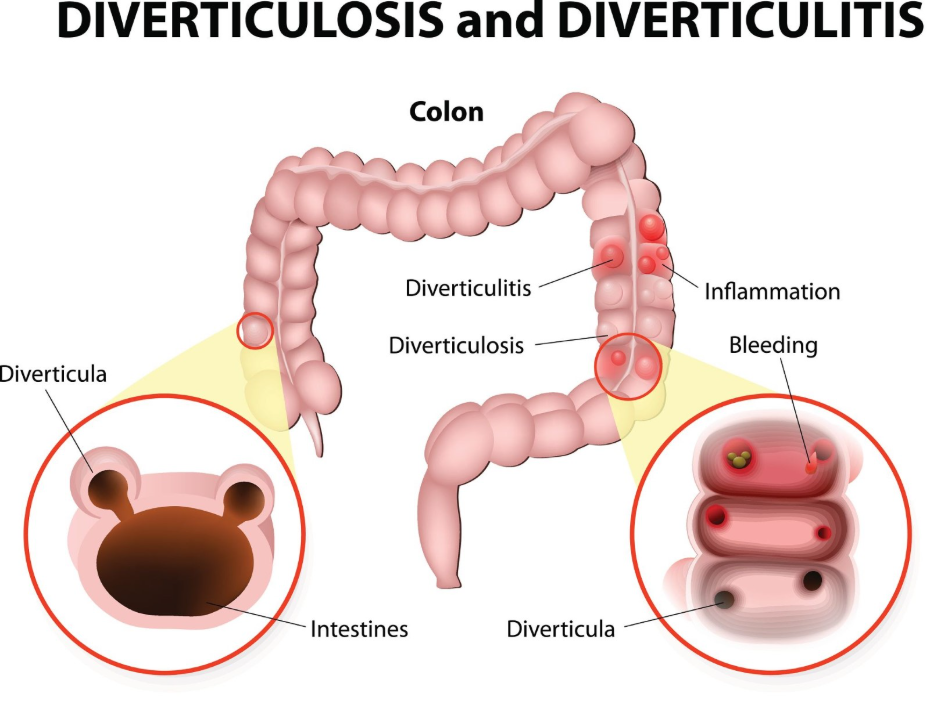
An abscess is a common complication of diverticulitis that occurs when the body’s immune system attempts to wall off a bacterial infection within or around an inflamed diverticular pouch. This results in a localised collection of pus and infected debris that can cause significant pain, persistent fever, and a palpable mass in the abdomen. The NHS states that diverticulitis can lead to complications such as an abscess, which is a collection of pus that may require drainage.
In the United Kingdom, clinicians typically use a CT scan to determine the size and location of an abscess. Small abscesses may sometimes resolve with intensive antibiotic therapy and bowel rest. However, larger collections may require a procedure known as percutaneous drainage, where a radiologist uses imaging guidance to insert a small tube through the skin to drain the fluid. If left untreated, an abscess can rupture, leading to a more widespread and dangerous infection. The management goal in UK hospitals is to stabilise the patient and resolve the infection before it can lead to a perforation of the bowel wall.
Understanding the Risk of Bowel Perforation
A bowel perforation is a serious complication where a hole develops in the wall of the large intestine at the site of an inflamed diverticulum, often due to the extreme pressure of an infection or the thinning of the tissue. This structural failure allows bacteria, waste, and gas to escape from the colon into the sterile environment of the peritoneum. NICE clinical guidelines for diverticular disease management identify perforation as a medical emergency that requires immediate clinical assessment and often surgical intervention.
When a perforation occurs, the pain usually becomes sudden, severe, and widespread across the entire abdomen. The body’s inflammatory response to the leaked material can lead to peritonitis, a life-threatening infection of the abdominal lining. In UK emergency departments, clinicians remain highly vigilant for red-flag signs such as a rigid abdomen, high fever, and signs of sepsis. The immediate priority for a suspected perforation is surgical consultation and the administration of intravenous fluids and broad-spectrum antibiotics. Depending on the severity of the tear, emergency surgery may be necessary to repair the hole or remove the affected section of the colon.
The Relationship Between Perforation and Peritonitis
Peritonitis is the widespread inflammation of the lining of the abdominal cavity that occurs as a direct result of a perforated diverticulum, representing one of the most severe escalations of diverticulitis. Once the intestinal barrier is breached, the peritoneum reacts violently to the presence of foreign bacteria and waste products. This condition leads to a rapid decline in the patient’s stability, often involving a fast heart rate, low blood pressure, and extreme abdominal tenderness.
In the United Kingdom, peritonitis caused by diverticular perforation is graded using systems such as the Hinchey classification, which helps surgeons determine the appropriate level of intervention. If the leak is contained by surrounding organs, it may be managed more conservatively; however, if there is free-flowing waste in the abdomen, it constitutes a surgical emergency. The UK healthcare pathway ensures that patients with these symptoms are fast-tracked for diagnostic imaging and surgical review. Resolving peritonitis involves not only addressing the hole in the bowel but also thoroughly cleaning the abdominal cavity to prevent recurrent infection and systemic organ failure.
Comparative Overview of Diverticular Complications
Complications arising from diverticulitis differ in their clinical presentation and the level of urgency required for treatment.
| Complication | Physical Description | Common UK Management |
| Abscess | Localised collection of pus. | Antibiotics or image-guided drainage. |
| Perforation | A hole or tear in the bowel wall. | Emergency surgery or intensive monitoring. |
| Peritonitis | Widespread abdominal infection. | Urgent surgery and peritoneal washout. |
| Bowel Obstruction | Narrowing caused by scarring/swelling. | Bowel rest, fluids, or surgical bypass. |
| Fistula | Abnormal tunnel between organs. | Elective surgical repair. |
This table illustrates that while all these issues stem from the same underlying diverticular disease, they represent different stages of structural failure or infectious spread. In the UK, clinicians use this distinction to prioritise resources, ensuring that those with acute structural failures like perforation receive the most rapid response.
Long-term Complications: Fistulas and Obstructions
Chronic or recurrent episodes of diverticulitis can lead to long-term complications such as fistulas or bowel obstructions due to the accumulation of scar tissue and persistent inflammation. A fistula is an abnormal connection that forms between the colon and another nearby organ, such as the bladder or the small intestine. This occurs when an abscess or an area of deep inflammation erodes through the walls of both structures.
The GOV.UK health pages indicate that complicated diverticular disease may require long-term surgical planning to address issues like fistulas that significantly impact quality of life. A bowel obstruction happens when repeated bouts of inflammation cause the bowel wall to thicken and scar (fibrosis), eventually narrowing the passage so much that waste cannot pass through. Both conditions typically require elective surgical intervention once the acute infection has been controlled. In the UK, patients with these chronic complications are managed by specialist colorectal teams who weigh the risks of surgery against the ongoing symptoms to find the most sustainable long-term solution.
UK Clinical Pathways for Complicated Diverticulitis
The management of complicated diverticulitis in the United Kingdom follows a rigorous pathway designed to identify the exact nature of the complication through advanced imaging before deciding on a treatment strategy. If a patient presents with severe abdominal pain, the first step in a UK hospital is usually a CT scan of the abdomen and pelvis with contrast. This scan allows radiologists to see the “fat stranding” of inflammation, the fluid of an abscess, or the free air of a perforation.
Based on the scan results, the patient is assigned to a specific care level. Uncomplicated cases may be treated with home rest and fluids, whereas complicated cases involving an abscess or perforation require hospitalisation. The UK clinical approach has shifted in recent years toward more conservative management of some perforations if they are small and contained, but surgical readiness remains a priority. Post-recovery, patients are often followed up with a colonoscopy several weeks later to ensure the bowel has healed and to rule out other issues like polyps. This integrated approach ensures that the immediate life-threatening risks are managed while the long-term health of the colon is protected.
Conclusion
Diverticulitis can lead to significant complications such as abscesses, perforations, and peritonitis, all of which require prompt clinical evaluation. While an abscess involves a localised infection that may be drained, a perforation is a structural failure of the bowel wall that can lead to widespread abdominal infection. In the UK, these complications are staged using CT imaging and managed through a combination of antibiotics, specialised drainage, or surgery. Recognising red-flag symptoms and following a structured care pathway are essential for preventing long-term damage like obstructions or fistulas. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
How common are these serious complications?
Most people with diverticulitis do not develop complications, but approximately 15% to 20% may experience issues like an abscess or perforation during a flare-up.
Can a perforation heal on its own without surgery?
Very small, “contained” perforations can sometimes be managed with antibiotics and hospital monitoring, but many require surgical repair.
What are the signs that an abscess has formed?
Persistent fever despite taking antibiotics and a tender lump in the abdomen are common signs that an abscess may be present.
Will I need a stoma bag if I have a perforation?
In some emergency surgeries for perforation, a temporary stoma is needed to allow the bowel to heal, but this is often reversed in a later procedure.
Can a high-fibre diet prevent these complications?
A high-fibre diet is recommended to prevent diverticula from forming and becoming inflamed, but it should be avoided during an active, painful flare-up.
What is a fistula exactly?
A fistula is an abnormal tunnel that links the colon to another organ, like the bladder, often causing symptoms such as recurrent urinary infections.
How long does it take to recover from complicated diverticulitis?
Recovery depends on the treatment; hospital stays for an abscess or perforation may last several days, with full recovery taking several weeks.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the complications of diverticulitis, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with extensive experience in emergency care, surgery, and general medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


