

Smoking significantly increases the risk of developing both colon polyps and diverticulitis by introducing systemic toxins that disrupt cellular health and impair the blood supply to the intestinal tissues. While colon polyps are abnormal tissue growths on the inner lining of the bowel, diverticulitis involves the inflammation or infection of small pouches that bulge outward from the colon wall. Although these conditions involve different biological processes, they are both negatively impacted by the chemical compounds found in tobacco smoke, which promote inflammation and oxidative stress throughout the gastrointestinal tract. In the United Kingdom, healthcare professionals identify smoking as a major modifiable risk factor for various bowel conditions, as it can accelerate the formation of growths and increase the likelihood of painful inflammatory flare-ups. Understanding the link between tobacco use and structural changes in the large intestine is a vital component of preventative healthcare. By addressing the impact of smoking on the colon, the UK healthcare system aims to reduce the incidence of serious bowel complications and support long-term digestive stability.
What We’ll Discuss in This Article
- The impact of tobacco toxins on the development of colon polyps.
- How smoking impairs blood flow and increases diverticulitis risk.
- The relationship between smoking and the severity of bowel inflammation.
- Comparing the risks of cellular overgrowth versus tissue infection.
- Long-term benefits of smoking cessation for gastrointestinal health.
- UK clinical guidance on managing lifestyle risks for the colon.
Smoking and the Development of Colon Polyps
Smoking increases the risk of colon polyps by exposing the bowel lining to carcinogens that cause DNA mutations and interfere with the body’s natural cell renewal cycles. The cells lining the colon are constantly dividing to replace old tissue; when tobacco toxins enter the bloodstream, they can damage the genetic material responsible for regulating this division. The NHS states that bowel polyps are caused by an overgrowth of cells in the lining of the large intestine and that smoking can increase the risk of developing them.
These cellular mutations can lead to the formation of adenomas, which are the type of polyps most likely to progress toward more serious conditions if left undetected. Research indicates that smokers tend to develop larger polyps and a higher number of growths compared to non-smokers. In the United Kingdom, clinicians prioritise regular bowel screening for individuals with a history of tobacco use because the chemical irritation from smoking makes the mucosal environment more susceptible to abnormal tissue growth. Removing these polyps early during a colonoscopy is essential for maintaining bowel health.
Impact of Smoking on Diverticulitis Risk
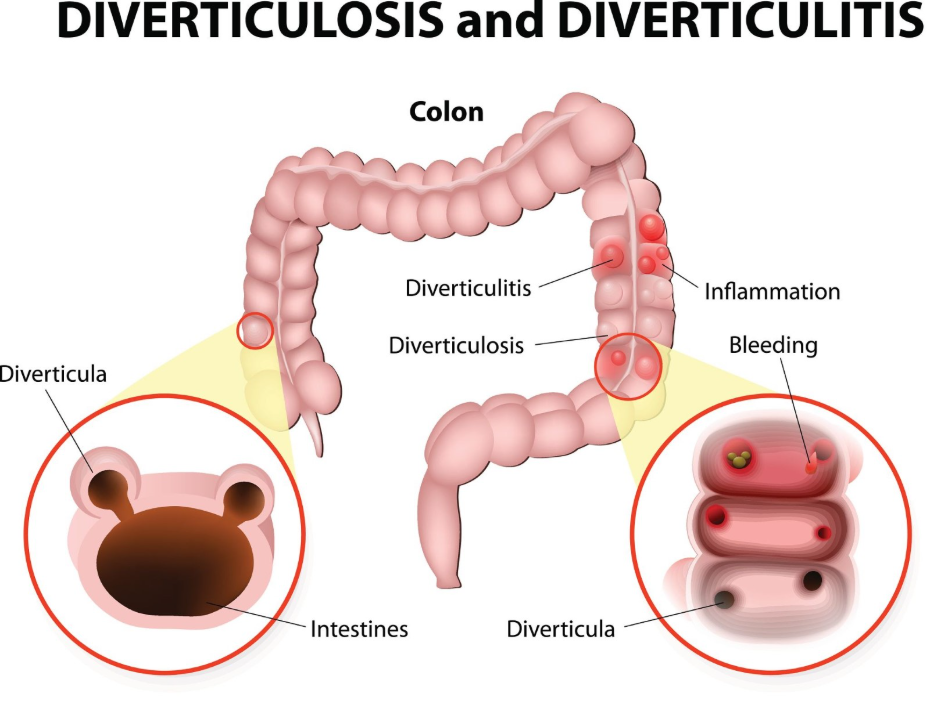
Smoking is a significant risk factor for diverticulitis because it impairs the blood supply to the colon wall and weakens the tissue, making the development and infection of diverticula more likely. Diverticulitis occurs when small pouches in the colon wall become inflamed or infected. Tobacco use causes vasoconstriction, which reduces the amount of oxygen and nutrients reaching the intestinal tissues.
NICE clinical guidelines for diverticular disease management identify smoking as a modifiable factor that increases the risk of symptomatic diverticulosis and acute diverticulitis flare-ups. When the blood supply is compromised, the bowel wall becomes less resilient to internal pressure, and the body’s ability to fight off localised infections within the pouches is diminished. Furthermore, smokers who develop diverticulitis are at a higher risk of experiencing complications, such as a perforated bowel or an abscess, compared to non-smokers. This increased vulnerability makes smoking cessation a primary recommendation for individuals already identified as having diverticula.
Inflammation and Oxidative Stress in the Bowel
Tobacco use promotes a state of chronic systemic inflammation that exacerbates the symptoms of diverticulitis and provides a fertile environment for the growth of polyps. The thousands of chemicals found in cigarette smoke trigger an immune response that increases the production of pro-inflammatory cytokines throughout the digestive tract.
In the context of diverticulitis, this heightened inflammatory state means that a minor irritation in a pouch can quickly escalate into a severe infection. For polyps, oxidative stress caused by smoking damages the antioxidants that normally protect the colon cells from injury. This chemical imbalance makes it easier for mutations to persist and for clusters of abnormal cells to expand. In the UK, healthcare providers emphasise that smoking does not just affect the lungs; its reach extends to the microscopic environment of the colon, where it disrupts the delicate balance of tissue repair and waste processing.
Comparison of Risks for Polyps and Diverticulitis
While smoking increases the risk for both conditions, the nature of the damage it causes differs between cellular overgrowth and structural infection.
| Feature | Colon Polyps | Diverticulitis |
| Primary Mechanism | Genetic mutations in the bowel lining. | Impaired blood flow and weakened wall. |
| Growth Type | Inward protrusion of tissue. | Outward bulging pouch (inflamed). |
| Complication Risk | Progression to malignancy. | Abscess, perforation, or obstruction. |
| Clinical Focus | Early detection via screening. | Resolving infection and preventing tears. |
This table illustrates that smoking affects the colon in two distinct ways: by attacking the DNA of the lining (polyps) and by weakening the structural integrity of the wall (diverticulitis). Both pathways lead to a higher burden of gastrointestinal disease, necessitating more frequent medical monitoring and intervention for current or former smokers in the UK.
Long-term Benefits of Smoking Cessation
Stopping smoking significantly reduces the risk of developing new colon polyps and helps protect the colon wall from the acute inflammatory episodes associated with diverticulitis. Once a person quits smoking, the body begins to repair the vascular damage, improving blood flow to the large intestine and enhancing the immune system’s ability to manage bacteria in the gut.
While existing diverticula will not disappear, the risk of them becoming infected decreases as the tissue health improves. Similarly, while cessation does not remove existing polyps, it lowers the rate at which new mutations occur in the bowel lining. The GOV.UK health pages indicate that smoking cessation is one of the most effective ways for individuals to improve their long-term digestive health and reduce their risk of bowel cancer. In the UK, patients with a history of bowel issues are strongly encouraged to utilise smoking cessation services to provide their colon with the best possible environment for recovery and stability.
UK Clinical Guidelines and Lifestyle Management
The UK healthcare system integrates smoking status into the assessment of bowel health, using this information to tailor screening and management plans for patients. During a clinical review for abdominal symptoms, a GP or specialist will often ask about tobacco use to gauge the likelihood of complications such as complicated diverticulitis or high-risk polyps.
Patients are supported through a holistic approach that includes dietary advice such as increasing fibre intake alongside lifestyle changes like quitting smoking. This multi-faceted strategy ensures that both the mechanical pressures on the colon (managed by fibre) and the chemical stresses (managed by stopping smoking) are addressed. Consistent participation in the national bowel screening programme is particularly vital for smokers, as they may be more prone to the “silent” development of growths. By managing these modifiable risks, individuals can work with their healthcare teams to maintain a functional and healthy colon throughout their lives.
Conclusion
Smoking increases the risk of colon polyps and diverticulitis by damaging the DNA of the bowel lining and impairing the blood supply to the intestinal wall. This habit makes the body more susceptible to cellular overgrowths and serious inflammatory complications like bowel perforations. In the UK, managing these risks involves a combination of regular screening and lifestyle modifications, including smoking cessation. Protecting the colon from tobacco-related toxins is an essential step in maintaining long-term gastrointestinal health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does vaping have the same risk for polyps as smoking?
The long-term effects of vaping on the colon are still being studied, but nicotine itself can affect blood flow to the bowel tissues.
If I quit smoking, will my diverticula go away?
No, diverticula are permanent structural changes, but quitting smoking will significantly reduce your risk of them becoming inflamed or infected.
Are smokers more likely to have painful colonoscopies?
Smoking can affect how the body processes certain medications used during procedures, but the medical team will manage this to ensure your comfort.
How long after quitting does my bowel risk decrease?
Your cardiovascular and inflammatory health begins to improve almost immediately, though the risk of polyps decreases more gradually over several years.
Can smoking cause blood in the stool?
Smoking does not cause bleeding directly, but it increases the risk of polyps and diverticular issues that can cause visible or microscopic blood.
Is the risk the same for light smokers?
Any amount of tobacco use increases the risk of bowel damage, although the risk is generally higher for those who have smoked more over a longer period.
Should I have screening earlier if I am a smoker?
In the UK, you should follow the standard age-based national screening programme unless your GP advises otherwise based on your symptoms or family history.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the impact of smoking on colon polyps and diverticulitis, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine, general surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
