


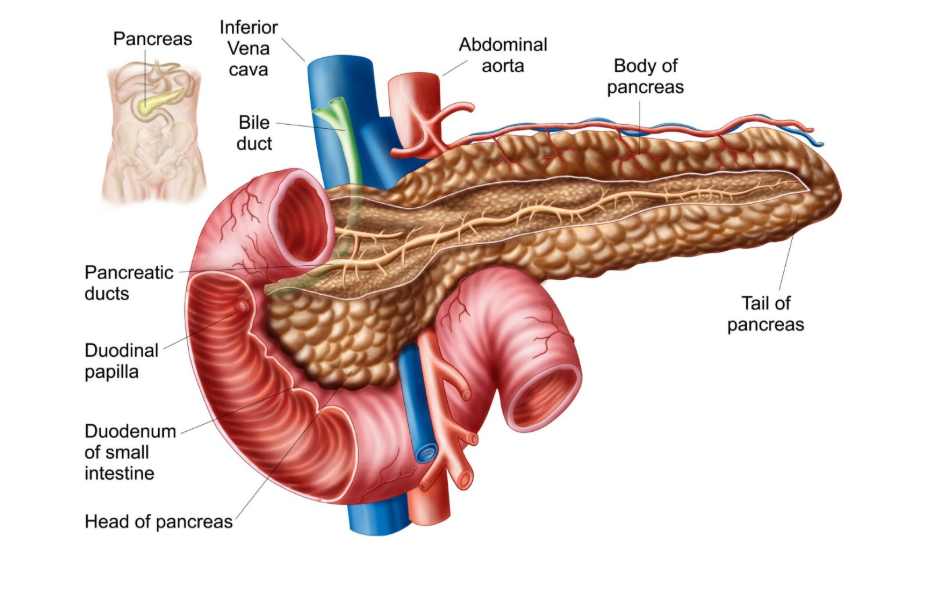
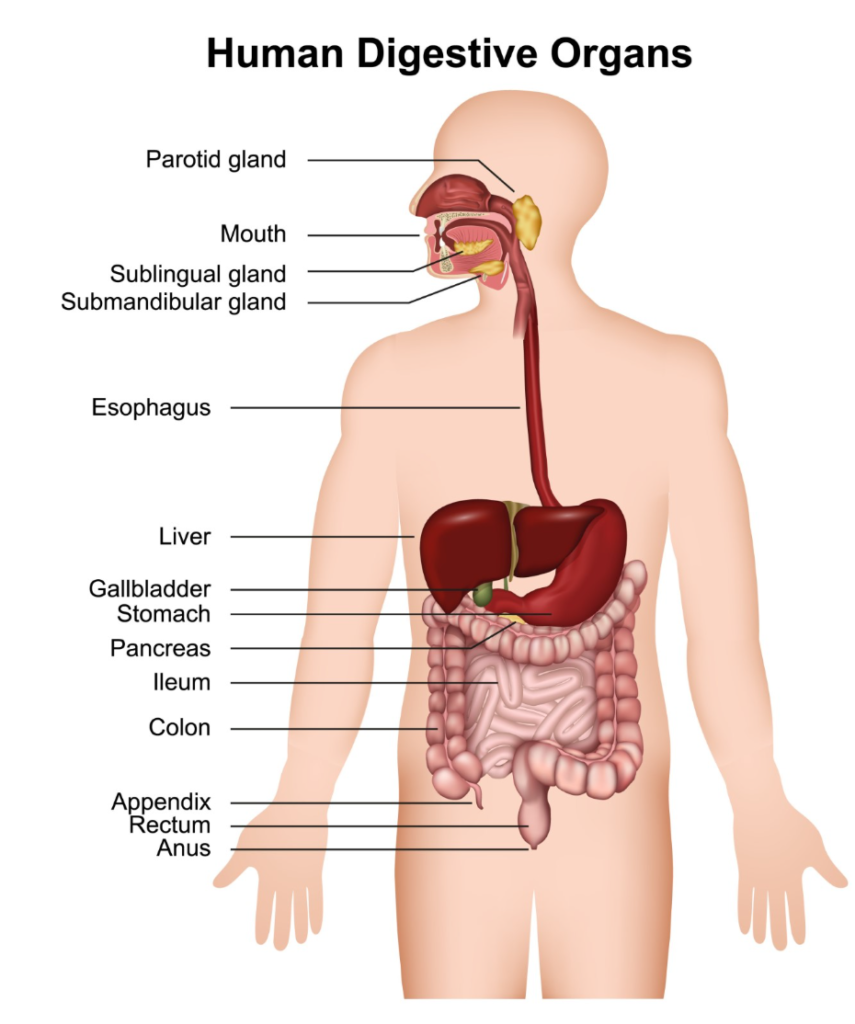
Pancreatitis and pancreatic infection are distinct medical occurrences, though they are often closely linked within a clinical setting. Pancreatitis refers to the inflammation of the pancreas, an organ situated behind the stomach that is essential for digestion and blood sugar regulation. This inflammation occurs when digestive enzymes become active while still inside the organ, causing it to begin digesting its own tissue. A pancreatic infection, on the other hand, is a potential complication that can arise during an episode of severe pancreatitis, particularly if part of the organ tissue dies due to a lack of blood supply. In the United Kingdom, healthcare professionals must carefully distinguish between sterile inflammation and an active infection, as the treatment pathways for each are significantly different. While initial management of pancreatitis focuses on supportive care and resting the organ, the presence of an infection necessitates the use of targeted antibiotics and potentially surgical intervention. Understanding these differences is vital for patients to comprehend their hospital care and the steps taken by medical teams to prevent the progression of the condition. By adhering to the evidence based standards set by the NHS and the National Institute for Health and Care Excellence, clinicians can monitor these transitions and provide the necessary interventions at the appropriate time.
What We’ll Discuss in This Article
- The biological definition of sterile inflammation versus infection
- How acute pancreatitis can progress to an infected state
- The role of pancreatic necrosis in developing an infection
- Diagnostic methods used in the UK to identify bacteria in the pancreas
- Treatment differences between standard pancreatitis and pancreatic infection
- Symptoms that may indicate a transition to an infectious complication
- Long term outcomes and the importance of early clinical intervention
Pancreatitis is the inflammation of the pancreas and is not the same as an infection, although an infection can develop as a serious complication of severe pancreatitis
Most cases of pancreatitis in the United Kingdom begin as sterile inflammation, meaning that no bacteria or viruses are initially involved in the process. Pancreatitis is inflammation of the pancreas, which can be acute or chronic and is often caused by gallstones or alcohol. The condition is triggered when the organ’s own digestive enzymes cause chemical damage to the tissue. An infection only occurs if bacteria manage to enter the inflamed or damaged parts of the pancreas, typically several days or weeks after the initial inflammation has started. Within the UK medical system, clinicians treat initial pancreatitis with fluids and pain relief, but they remain vigilant for signs of an infection, which is a much more critical and life threatening development.
The relationship between necrosis and infection
Pancreatic infection almost exclusively occurs in cases of severe acute pancreatitis where part of the organ has undergone necrosis, which is the death of tissue. When the inflammation is so intense that the blood supply to sections of the pancreas is cut off, that tissue dies and becomes a breeding ground for bacteria.
In severe cases of acute pancreatitis, the pancreas can lose its blood supply, which can lead to some of the tissue dying and becoming infected. This infected necrosis is one of the most serious complications of the condition. In the UK, specialists use contrast enhanced CT scans to identify areas of necrosis and monitor the patient for systemic signs of infection, such as a rising fever or an increased white blood cell count.
Identifying the transition from inflammation to infection
Distinguishing between the symptoms of sterile pancreatitis and an infection can be challenging because both cause severe abdominal pain and a general feeling of being unwell. However, an infection is often marked by a secondary decline in the patient’s condition after an initial period of stability. Symptoms such as a high temperature, shivering, and a rapid heartbeat that do not improve with standard supportive care may suggest that bacteria have invaded the pancreatic tissue. According to the National Institute for Health and Care Excellence, healthcare professionals should suspect an infection if a patient with severe pancreatitis develops new signs of sepsis or fails to improve after the first week. Prompt identification is essential because an infection significantly increases the risk of multi organ failure and requires a shift in the clinical management strategy.
Diagnostic investigations for pancreatic infection
In the United Kingdom, doctors use specific tests to determine if a patient’s pancreatic issues have progressed to an infection. If a CT scan shows gas bubbles within the necrotic tissue of the pancreas, this is a strong indicator of bacterial activity. In some cases, a procedure called fine needle aspiration may be performed, where a small sample of fluid is taken from the pancreas using a needle guided by a scan to be tested for bacteria in a laboratory. These investigations help the medical team decide whether to start a course of intravenous antibiotics. Unlike many other inflammatory conditions, antibiotics are not routinely given for simple pancreatitis and are reserved for when an infection is either proven or highly suspected.
Comparison of Inflammation and Infection in the Pancreas
| Feature | Pancreatitis (Inflammation) | Pancreatic Infection |
| Primary Trigger | Premature enzyme activation | Bacterial invasion of dead tissue |
| Typical Timing | Sudden onset at the start | Usually 1 to 4 weeks after onset |
| Antibiotics | Not usually required | Essential (often intravenous) |
| Necrosis | May or may not be present | Almost always present |
| Main Treatment | IV fluids, pain relief, rest | Antibiotics, possible drainage/surgery |
Treatment pathways for pancreatic infection
The management of an infected pancreas is considerably more complex than the treatment for standard pancreatitis. In the UK, if an infection is confirmed, the patient will receive broad spectrum antibiotics that can penetrate the pancreatic tissue. If the patient does not respond to medication alone, a procedure to drain the infected fluid or remove the dead, infected tissue may be necessary. This can often be done using minimally invasive techniques, such as placing a drain through the skin under the guidance of a scan, rather than traditional large scale surgery. The goal of UK clinical teams is to clear the infection and stabilise the patient’s organ function while allowing the rest of the pancreas time to heal from the initial inflammatory damage.
Complications and long term recovery
A pancreatic infection is a serious event that can prolong a hospital stay by several weeks or months and may lead to long term functional changes in the organ. If a large portion of the pancreas is damaged by infection and necrosis, the patient may develop permanent issues such as diabetes or difficulty digesting food. During recovery in the UK, patients are monitored by a multidisciplinary team to manage these long term consequences. Early intervention and the careful use of diagnostic imaging have improved the outlook for patients with these complications, but avoiding the primary triggers of pancreatitis, such as gallstones and excessive alcohol, remains the best way to prevent these severe infectious outcomes.
Conclusion
Pancreatitis is an inflammatory condition that is fundamentally different from a pancreatic infection, though the two can occur sequentially. Infection is a severe complication that usually involves bacteria invading dead pancreatic tissue known as necrosis. Treatment in the UK focuses on distinguishing between these states to ensure that antibiotics and drainage are only used when clinically necessary. Recognising the signs of a worsening condition is essential for early intervention and better recovery outcomes. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can you get a pancreatic infection without having pancreatitis first?
It is extremely rare; almost all pancreatic infections occur as a secondary complication following an episode of severe acute pancreatitis.
Do I always need antibiotics if my pancreas is inflamed?
No, in the UK, antibiotics are only prescribed if there is evidence or a very high suspicion of an infection, as they do not help with sterile inflammation.
How do doctors know if the tissue in my pancreas has died?
Clinicians use a CT scan with a special dye (contrast) to see if blood is still reaching all parts of the organ; areas without blood flow are considered necrotic.
Is an infected pancreas contagious?
No, a pancreatic infection is an internal complication and cannot be passed from one person to another.
Will I need surgery if I have a pancreatic infection?
Not always; many infections are managed with antibiotics or by placing a small drain through the skin to remove infected fluid.
How long does it take for an infection to show up?
A pancreatic infection typically develops between one and four weeks after the start of the initial pancreatitis episode.
Can a pancreatic infection cause diabetes?
If the infection and associated tissue death affect the parts of the pancreas that make insulin, it can lead to permanent blood sugar issues.
Authority Snapshot (E-E-A-T Block)
This article was developed by the Medical Content Team to provide clear education on the complexities of pancreatic health and complications. The content has been reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery and emergency medicine, to ensure absolute alignment with NHS and NICE clinical guidance. Our purpose is to help the public understand the difference between inflammation and infection through factual and restrained reporting.


