


Schizophrenia is not the same as being dangerous or violent because the vast majority of individuals living with this condition are more likely to be victims of crime or harm themselves rather than pose a threat to others. In the United Kingdom, healthcare professionals focus on a recovery-based model that prioritises biological stability through integrated NHS support. Most people with schizophrenia manage their symptoms effectively within the community while maintaining stable social and professional lives.
What We’ll Discuss in This Article
- The clinical reality of schizophrenia versus common social misconceptions.
- Biological drivers of symptoms and their impact on functional behaviour.
- Research regarding risk factors and the prevalence of harm in the UK.
- Identifying the physical and psychological markers of clinical stability.
- The role of integrated NHS care pathways in maintaining patient safety.
- Accessing multidisciplinary support through specialist community mental health teams.
Clinical Reality Versus Social Misconceptions
Schizophrenia is a complex neurological and psychological condition characterised by changes in perception and thought processing, but it is not a predictor of dangerous or violent behaviour toward the public. In the United Kingdom, clinical evidence suggests that stigma and media portrayals often create an exaggerated perception of risk that does not align with the experiences of most patients. The NHS states that most people with schizophrenia are not violent and are more likely to be victims of violence than perpetrators.
When an individual receives consistent care, their symptoms are typically managed through a combination of pharmacological and psychological interventions. In the UK, this professional framework provides a stable foundation for the health journey by identifying that behaviour is influenced by biological and environmental factors. By utilised these integrated pathways, the healthcare system ensures that every person’s profile is supported through evidence-based understanding. This coordinated effort prioritises the safety of the individual within a validated medical environment.
Biological Drivers of Symptoms and Behaviour
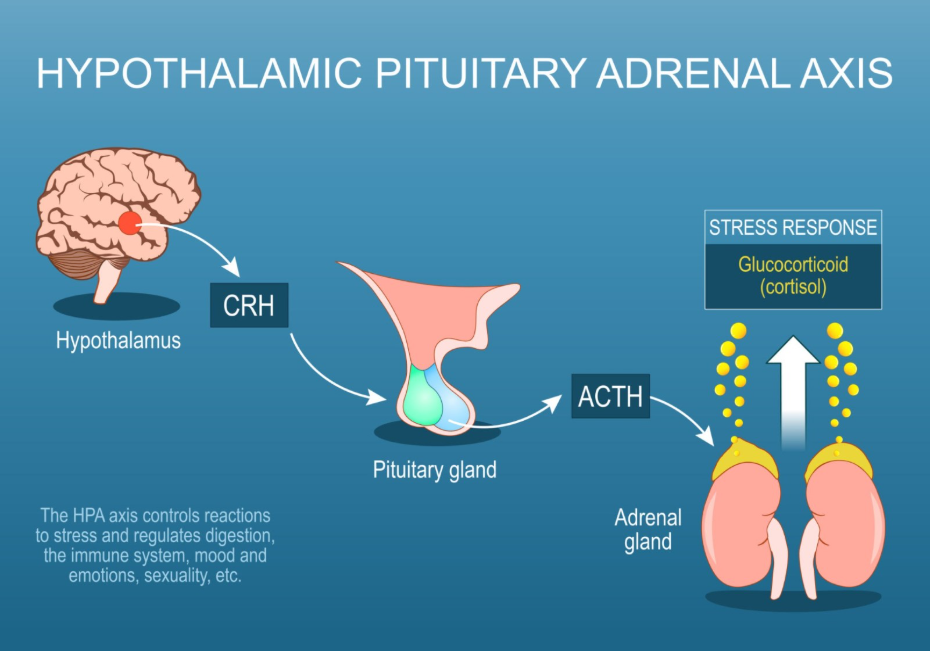
The symptoms of schizophrenia, such as hallucinations or delusions, result from neurochemical changes in the brain, specifically involving dopamine regulation, but these experiences rarely lead to aggressive actions toward others. In the United Kingdom, specialists recognise that individuals experiencing acute psychosis are often in a state of intense fear or confusion rather than hostility. NICE clinical guidelines for psychosis and schizophrenia indicate that a thorough assessment should focus on the individual’s safety and the reduction of distress.
| Symptom Category | Biological Mechanism | Functional Impact |
| Hallucinations | Perceptual changes in auditory or visual processing. | Increased internal distress and social withdrawal. |
| Delusions | Fixed beliefs not aligned with external reality. | Potential for confusion or feeling under threat. |
| Cognitive Shifts | Changes in executive function and memory. | Difficulty in planning or managing daily tasks. |
| Negative Symptoms | Reduced emotional expression or motivation. | Social isolation and leaden physical heaviness. |
| Disorganised Thought | Fragmentation of logical communication. | Challenges in navigating complex social cues. |
In the UK, these biological changes are managed through integrated care plans that prioritise a person-centred approach. Identifying that perceptual shifts are biological responses to neurochemical dysregulation helps the multidisciplinary team select the most effective management strategy. This professional oversight is essential for providing a safe and accurate understanding of the individual’s functional capability. By building a robust evidence base through clinical review, the healthcare system provides a secure environment for long-term health.
Research on Risk Factors and Victimisation
Research in the United Kingdom indicates that the risk of harm is significantly higher for the person with schizophrenia themselves, through self-harm or neglect, than for the people around them. Healthcare professionals identify that specific external factors, such as substance misuse or a lack of clinical engagement, are better predictors of agitation than the condition itself. The GOV.UK health pages provide clinical profiles indicating that the monitoring of social and cognitive challenges is a priority for ensuring integrated support.
When individuals are effectively supported by community mental health teams, the likelihood of any destabilisation is greatly reduced. In the UK, the focus is on providing a stable foundation where the individual’s environment is reviewed alongside their metabolic health. Identifying these underlying drivers allows for more targeted help that addresses the actual biological cause of distress. By utilised these professional frameworks, the UK system provides a life-long framework of support that adapts to the person’s needs.
Identifying Markers of Clinical Stability
Identifying the markers of clinical stability involves looking for a combination of physical and psychological indicators that suggest the nervous system is responding well to management. In the United Kingdom, healthcare professionals focus on how these improvements reflect the individual’s ability to participate in their community and maintain their social roles.
Common markers of stability identified in the UK include:
- Symptom Regulation: A reduction in the frequency or intensity of perceptual disturbances.
- Routine Maintenance: Consistency in personal hygiene, nutrition, and home environment.
- Social Participation: Engaging with friends, family, or community groups comfortably.
- Biological Regulation: Stable sleep patterns and regulated autonomic nervous system arousal.
- Insight and Awareness: Ability to recognise changes in health and seek clinical review early.
- Occupational Stability: Participating in work, volunteering, or educational opportunities.
In the UK, identifying these indicators early is vital for preventing the functional decline that often accompanies chronic health challenges. The integrated support framework encourages a strengths-based approach, focusing on what the individual needs to remain healthy. By utilised these professional frameworks, the healthcare system provides a secure environment for building professional and personal confidence. These strategies aim to work with the individual’s biology to restore a sense of calm.
Accessing Integrated NHS Support Pathways
The pathway for managing schizophrenia in the United Kingdom is a coordinated process involving specialist teams such as Early Intervention in Psychosis or Community Mental Health Teams. This journey ensures that every individual receives a thorough review of their history and current environment to build a bespoke recovery plan that supports their long-term wellness.
The UK integrated support pathway involves:
- Care Coordination: Having a named professional to manage all aspects of clinical and social care.
- Specialist Assessment: Undergoing regular multidisciplinary reviews with psychiatrists and nurses.
- Talking Therapies: Accessing evidence-based support such as Cognitive Behavioural Therapy for psychosis.
- Physical Health Monitoring: Annual checks of weight, blood pressure, and metabolic markers.
- Stay-Well Planning: Creating a relapse prevention plan that identifies early warning signs.
- Family Support: Providing education and sessions for relatives to foster a supportive home.
In the UK, the focus is on providing a stable foundation for the individual to move forward with self-understanding. The NHS ensures that adults have a consistent point of contact for their health needs while they navigate their lives. By utilised these integrated pathways, the healthcare system provides a secure environment for building long-term mental wellbeing across the UK population. These strategies aim to work with the individual’s biology to restore a sense of calm and purpose.
Conclusion
Schizophrenia is a health condition that does not equate to being dangerous or violent, as clinical evidence in the United Kingdom confirms that individuals with this condition are far more vulnerable than they are a threat. The NHS and professional bodies provide a robust system of multidisciplinary care to help individuals achieve stability and maintain their functional independence. By focusing on both the biological roots of symptoms and the need for supportive environments, the system promotes the highest possible level of safety and recovery. Following a coordinated management plan with the help of medical and psychological experts ensures that unique adult and paediatric needs are addressed holistically.
Are people with schizophrenia unpredictable?
Most individuals follow predictable patterns of health, and any changes are usually identified early through regular NHS clinical reviews.
Does medication help prevent agitation?
Yes; antipsychotic medication helps achieve neurochemical stability, which reduces the distress and confusion that can sometimes lead to agitation.
What should I do if a loved one seems confused?
You should contact their care coordinator or GP for a clinical review to ensure they have the appropriate support for their symptoms.
Is victimisation common for those with schizophrenia?
Unfortunately, people with severe mental health conditions in the UK are statistically more likely to experience crime or social exclusion.
Can people with schizophrenia live independently?
Yes; with integrated support from the NHS and social services, many people live independently and manage their daily lives successfully.
Why is there such a strong link between the condition and violence in the news?
Social stigma and rare, extreme cases often receive more attention than the millions of people who live stable lives with the condition.
Who should I talk to first to learn more?
The first point of contact in the United Kingdom is usually your GP or your local community mental health team.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding schizophrenia and behaviour, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in multiple clinical specialties including emergency care, general medicine, and medical education. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


