

Diverticulitis is a medical condition characterised by the inflammation or infection of small, bulging pouches called diverticula that develop in the lining of the large intestine. These pouches, which form due to pressure on weakened areas of the bowel wall, are common as people age and are collectively referred to as diverticulosis. While many individuals live with diverticulosis without experiencing symptoms, diverticulitis occurs when these pouches become obstructed or inflamed, leading to acute abdominal pain and systemic signs of infection. In the United Kingdom, healthcare professionals manage this condition with a focus on resolving the immediate inflammation and providing long-term dietary guidance to prevent recurrence. The impact on the colon can range from localised swelling to more serious complications if the infection is not managed effectively. Understanding the biological transition from having pouches to experiencing active inflammation is essential for patients to recognise when clinical intervention is required. By managing bowel health through lifestyle and appropriate medical care, the complications associated with this condition can often be mitigated.
What We’ll Discuss in This Article
- The biological difference between diverticulosis and diverticulitis.
- The physical process of how diverticula form in the colon wall.
- Clinical symptoms and how inflammation affects bowel function.
- Common causes and risk factors associated with diverticular disease.
- Potential complications such as abscesses or bowel obstructions.
- UK clinical pathways for the diagnosis and management of flare-ups.
The Distinction Between Diverticulosis and Diverticulitis
Diverticulitis is specifically the active inflammatory or infectious stage of diverticular disease, whereas diverticulosis simply refers to the presence of the pouches without any symptoms. Most people in the UK over the age of fifty have some degree of diverticulosis, often discovered incidentally during unrelated bowel investigations. The NHS states that diverticular disease and diverticulitis are related conditions that affect the large intestine, with diverticulitis being the more serious of the two.
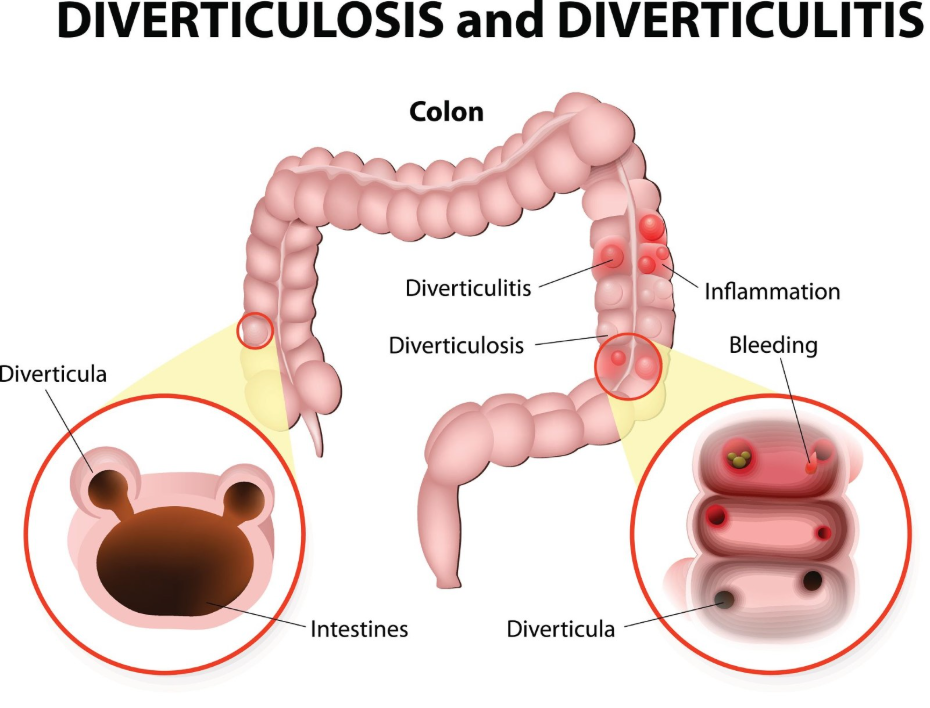
While diverticulosis is considered a structural change in the bowel wall, diverticulitis is a physiological crisis. The transition occurs when a diverticulum becomes blocked, possibly by waste matter or undigested food, which leads to bacterial overgrowth and subsequent tissue inflammation. In the UK healthcare system, clinicians use these terms distinctly to determine the level of urgency and the type of treatment required. Patients with diverticulosis are typically managed through dietary changes, while those with diverticulitis may require antibiotics or hospital-based supportive care to resolve the infection.
How Diverticula Form in the Bowel Wall
Diverticula form in the colon when high pressure within the bowel pushes the inner lining through weak spots in the outer muscle layer, creating small protrusions or pockets. This process is often linked to the way the colon moves waste; if the bowel has to exert significant force to move small or hard stools, the internal pressure increases.
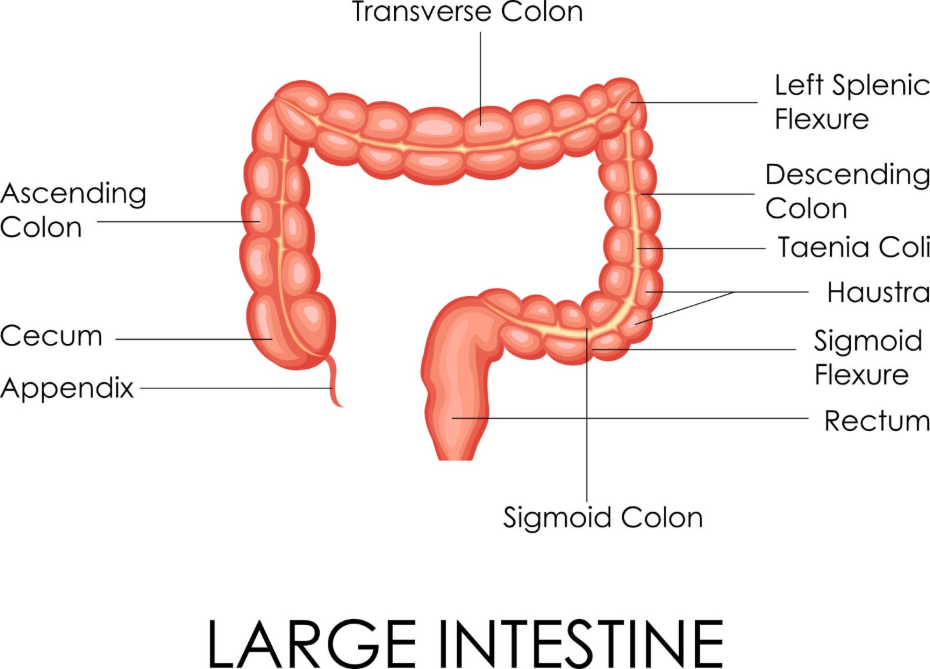
Over many years, this recurring pressure causes the mucosa, or inner lining, to herniate through the muscular wall, most commonly in the sigmoid colon, which is the lower left part of the large intestine. These pockets are typically between five and ten millimetres in size. Factors such as low dietary fibre are thought to contribute to this process by making the stools harder and more difficult to pass. In the United Kingdom, identifying these structural changes is a routine part of gastrointestinal health assessments, especially for individuals reporting changes in bowel habits.
How Inflammation Affects Colon Function
When a diverticulum becomes inflamed, it causes the surrounding tissue in the colon to swell, which can interfere with the normal movement of waste and lead to significant localised pain. This inflammation often presents as a sharp or cramping pain in the lower left side of the abdomen, though it can occur on the right side in some populations.
The swelling within the bowel wall can cause the colon to become sensitive and reactive, leading to changes in bowel habits such as constipation or diarrhoea. NICE clinical guidelines for diverticular disease management emphasise that the presence of systemic symptoms like fever and nausea alongside abdominal pain are key indicators of acute diverticulitis. During a flare-up, the colon’s ability to absorb water and move waste effectively is compromised, which is why UK clinicians often recommend a temporary clear fluid diet to allow the bowel to rest and the inflammation to subside before reintroducing solid foods.
Causes and Modifiable Risk Factors
The development of diverticulitis is influenced by a combination of non-modifiable factors like age and genetics, alongside modifiable lifestyle factors such as diet, weight, and physical activity levels. Age is a primary factor, as the muscle wall of the colon naturally loses elasticity and becomes weaker over time.
| Risk Factor | Impact on Colon Health | Preventative Action |
| Low Fibre Diet | Leads to harder stools and increased bowel pressure. | Increase intake of whole grains and vegetables. |
| Obesity | Associated with higher rates of inflammation in the bowel. | Maintain a healthy weight through diet and exercise. |
| Smoking | Impairs blood flow to the colon and delays healing. | Cessation of smoking to improve vascular health. |
| Physical Inactivity | Can slow down the passage of waste through the gut. | Regular moderate activity to support bowel motility. |
In the United Kingdom, public health advice focuses heavily on the role of fibre in maintaining soft stools and reducing the pressure within the colon. Additionally, certain medications, such as non-steroidal anti-inflammatory drugs, have been linked to an increased risk of diverticular complications. By addressing modifiable risks, individuals can lower the likelihood of diverticula forming and reduce the frequency of inflammatory flare-ups.
Potential Complications of Untreated Inflammation
If diverticulitis is not managed effectively, it can lead to more serious complications such as an abscess, a perforation of the bowel wall, or a blockage in the colon. An abscess is a localised collection of pus that forms near the inflamed pouch; if this rupture occurs, it can lead to peritonitis, which is a widespread and life-threatening infection of the abdominal lining.
Chronic or repeated episodes of inflammation can also lead to the formation of scar tissue, which may narrow the bowel lumen and cause a partial or total obstruction. The GOV.UK health pages indicate that monitoring for red-flag symptoms such as severe bleeding or persistent vomiting is essential for the early detection of these serious diverticular complications. In the UK, most cases of diverticulitis are uncomplicated and resolve with standard care, but these secondary issues require urgent surgical or radiological intervention to restore bowel integrity and prevent systemic illness.
UK Clinical Pathways for Diagnosis and Care
The diagnosis and management of diverticulitis in the United Kingdom follow a structured pathway that involves clinical assessment, blood tests to check for infection markers, and imaging to confirm the presence of inflammation. A CT scan is often the preferred imaging tool during an acute flare-up because it can accurately show the severity of the inflammation and identify any complications like abscesses.
Management in the UK is generally tailored to the severity of the symptoms. Uncomplicated diverticulitis is often managed at home with rest, fluids, and sometimes oral antibiotics. For more severe cases, hospital admission may be required for intravenous fluids and antibiotics. Once the acute phase has passed, UK clinicians provide long-term guidance on gradually increasing dietary fibre to help prevent future episodes. Colonoscopy is usually avoided during the acute inflammatory phase due to the risk of perforation, but it may be scheduled several weeks later to confirm the diagnosis and ensure the bowel is otherwise healthy.
Conclusion
Diverticulitis is a condition where small pouches in the colon lining become inflamed or infected, leading to pain and changes in bowel habits. While diverticulosis is a common part of ageing, the transition to diverticulitis requires prompt clinical attention to manage inflammation and prevent complications. In the UK, a combination of dietary adjustments and medical intervention is used to restore colon function and maintain long-term bowel health. Following clinical guidance on fibre intake and lifestyle management is the most effective way to reduce the risk of future flare-ups. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can I prevent diverticula from forming?
While you cannot change age-related weakening of the bowel, eating a high-fibre diet and drinking plenty of water can help keep bowel pressure low.
Should I avoid nuts and seeds if I have diverticulosis?
Current UK clinical guidance suggests there is no evidence that nuts or seeds cause diverticulitis, and they are actually a good source of fibre.
Is diverticulitis the same as irritable bowel syndrome?
No, diverticulitis involves physical inflammation or infection of pouches in the colon, whereas IBS is a functional disorder without visible inflammation.
Will I need surgery for diverticulitis?
Most cases are managed with diet and medication; surgery is generally only considered for serious complications like a perforated bowel or repeated severe attacks.
How long does a flare-up last?
With appropriate care, most people begin to feel better within a few days, though it can take a week or more for the inflammation to resolve completely.
Can diverticulitis cause blood in my stool?
Yes, diverticula can sometimes bleed; if you notice bright red blood in your stool, you should seek medical advice promptly.
What is a “low residue” diet?
This is a temporary diet low in fibre used during a flare-up to give the bowel a rest before gradually moving back to a high-fibre diet.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding diverticulitis and its impact on the colon, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine, general surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
