

If bowel cancer screening or diagnostic tests identify polyps or suspicious lesions, the primary course of action involves further clinical investigation and, in many cases, immediate removal or biopsy. These findings are common and do not necessarily indicate the presence of cancer, but they do require careful medical management to prevent future health complications. The UK healthcare system follows structured protocols to ensure that every finding is assessed accurately and that patients receive the appropriate level of follow-up care based on the specific nature of the lesion.
What We’ll Discuss in This Article
- The definition and significance of bowel polyps and lesions.
- The procedure for removing polyps during a colonoscopy.
- How tissue samples are analysed in a laboratory setting.
- The different types of polyps and their associated risks.
- Surveillance and follow-up schedules for high-risk findings.
- Communication of results and next steps in the care pathway.
Immediate Clinical Actions for Polyps or Lesions
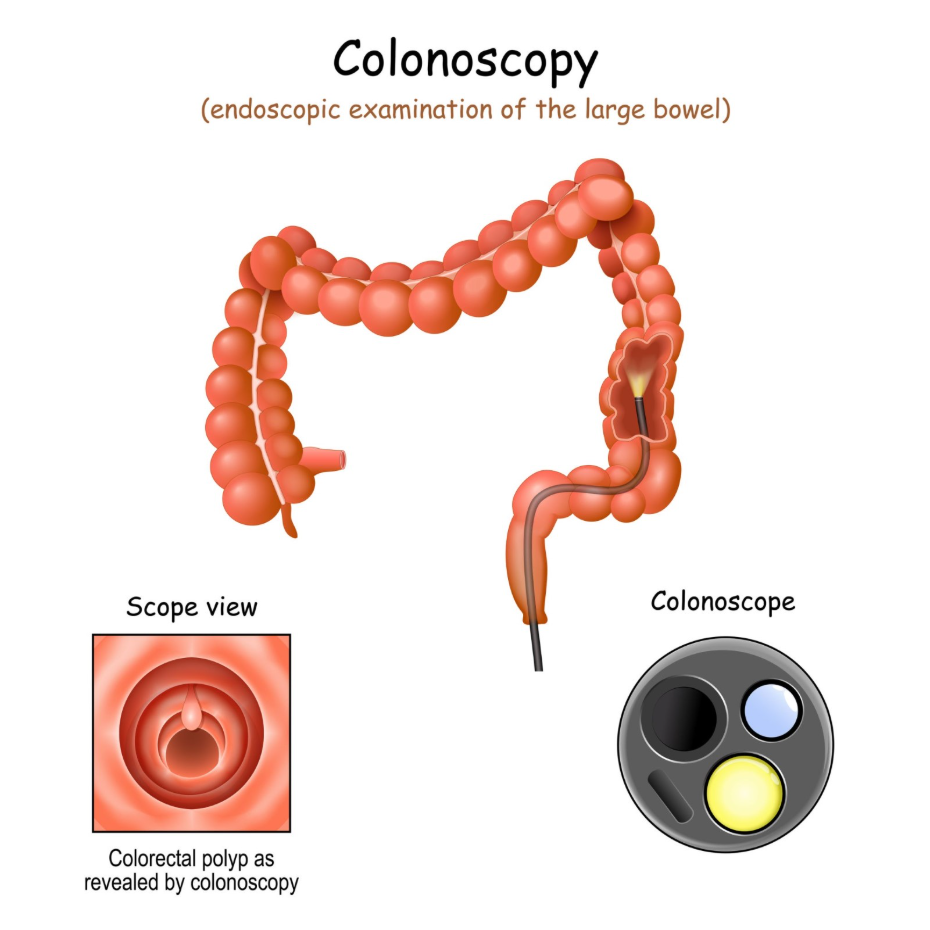
When a polyp or suspicious lesion is identified during a colonoscopy, the clinical team will usually attempt to remove it or take a tissue sample immediately. This proactive approach is a standard part of the procedure because many polyps, while initially benign, have the potential to develop into cancer over several years. Removing them effectively eliminates this risk before a more serious condition can develop.
The NHS bowel cancer screening programme ensures that any abnormalities found during a colonoscopy are managed by specialist clinicians to provide a clear diagnosis. If a lesion is too large to be removed during the initial procedure, or if its appearance suggests it requires more complex intervention, the clinician will take a biopsy. This involves taking a tiny piece of the tissue to be examined under a microscope, which helps the medical team decide the best secondary treatment plan.
The Process of Polypectomy and Biopsy
A polypectomy is the surgical removal of a polyp, typically performed during a colonoscopy using a wire loop or specialised forceps passed through the scope. The procedure is generally painless because the lining of the bowel does not have the same pain receptors as the skin. In some cases, an electric current is passed through the wire loop to cauterise the area, which helps prevent bleeding and ensures the entire growth is removed cleanly.
Once a polyp or lesion is removed, it is placed in a sterile container and sent to a pathology laboratory. NICE clinical guidelines state that all removed polyps should be histologically examined to determine their type and whether they contain any abnormal cells. This analysis is essential for determining the patient’s future risk level. While the visual appearance of a lesion can provide some clues, only a microscopic examination can confirm its exact biological characteristics.
Understanding Different Types of Polyps
Not all polyps carry the same level of risk, and the laboratory results will categorise them based on their growth pattern and cellular structure. The most common types are hyperplastic polyps and adenomas. Hyperplastic polyps are generally considered low risk and rarely become cancerous. Adenomas, however, are the type that clinicians monitor more closely as they are the precursors to the majority of bowel cancers.
The laboratory will also check for “dysplasia,” which describes how much the cells in the polyp look like cancer cells under a microscope. Low-grade dysplasia means the cells are only slightly abnormal, while high-grade dysplasia indicates that the cells are closer to becoming cancerous. This detailed classification is used to place the patient into a specific surveillance category, ensuring that those with higher-risk findings receive more frequent check-ups.
Post-Procedure Surveillance and Follow-Up
Following the removal of polyps or the identification of lesions, patients are assigned a follow-up schedule known as surveillance. This schedule is determined by the number, size, and type of polyps found. For individuals with low-risk findings, such as one or two small adenomas, they may simply be invited back to the standard national screening programme in two years.
For those with high-risk findings, such as large polyps or those showing high-grade dysplasia, the NHS provides more frequent hospital-based monitoring. This might involve a repeat colonoscopy after one, three, or five years. The table below outlines the general surveillance intervals used in the UK for different finding categories:
| Finding Category | Description | Typical Follow-up |
| Low Risk | 1–2 small adenomas (<10mm) | Return to regular screening |
| High Risk | At least 1 large adenoma (≥10mm) or 5+ small ones | Colonoscopy in 3 years |
| Complex Lesion | Large or difficult-to-remove growth | Follow-up in 6 to 12 months |
| Malignant Finding | Evidence of cancer in the lesion | Referral to multidisciplinary team |
Communication and Receiving Results
The final results from a polyp removal or biopsy usually take around two weeks to be processed by the pathology laboratory. Patients are typically informed of the initial findings immediately after their colonoscopy, but the definitive plan is only confirmed once the laboratory report is reviewed by the clinical team. Most hospitals will send a letter to both the patient and their GP explaining the results and the date for any future surveillance.
If a suspicious lesion is found to contain cancerous cells, the patient is referred to a multidisciplinary team (MDT). This team includes specialist surgeons, oncologists, radiologists, and nurses who work together to create a personalised treatment plan. Patients can access detailed information about the possible outcomes of a colonoscopy through official GOV.UK health resources. This ensures that individuals understand the implications of their results and the support available within the NHS.
Managing Symptoms After a Finding
It is important for individuals to remain aware of their bowel health even after polyps have been removed. While the removal of polyps significantly reduces the risk of cancer, it does not eliminate it entirely, especially if new growths develop between surveillance appointments. Patients should continue to monitor for persistent changes in bowel habits, unexplained weight loss, or new instances of rectal bleeding.
If any of these symptoms occur, they should be discussed with a healthcare professional promptly, regardless of when the next scheduled surveillance appointment is due. The clinical team that performed the colonoscopy will also provide specific instructions on what to look out for in the days immediately following a polypectomy, such as significant bleeding or severe abdominal pain, which may require urgent assessment.
Conclusion
Finding a polyp or lesion during bowel screening is an important step in preventing cancer and managing long-term health. Most polyps are successfully removed during the initial investigation, and subsequent surveillance ensures that any further changes are caught early. By following the recommended clinical pathway and attending all follow-up appointments, patients can significantly reduce their risk of developing bowel cancer. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
If my polyp was removed, am I now cured?
Removing a polyp eliminates that specific growth, but you may still be at risk of developing new ones, which is why surveillance is important.
Does having a polyp mean I will definitely get cancer?
No, most polyps never turn into cancer, but because it is impossible to tell which ones will, clinicians remove all adenomas as a precaution.
Can polyps grow back in the same spot?
While the original polyp is gone, a new one can occasionally grow in the same area or elsewhere in the bowel.
Is there a medication I can take to stop polyps from growing?
There is currently no standard medication used to prevent polyps in the general population, though a healthy diet and lifestyle are encouraged.
What if the doctor couldn’t remove the whole polyp?
If a polyp is too large or awkwardly placed, you may be referred for a specialised procedure or a minor operation to ensure it is fully removed.
Will I need surgery if I have a suspicious lesion?
Not necessarily; many lesions can be managed through endoscopy, but surgery is considered if the lesion is very large or shows signs of cancer.
How common is it to find polyps during a screening colonoscopy?
It is very common; polyps are found in approximately 40% to 50% of people who have a colonoscopy as part of the screening programme.
Authority Snapshot (E-E-A-T)
The information in this article is provided for educational purposes and is strictly aligned with the clinical protocols of the NHS and NICE. This content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with extensive clinical experience in surgery and diagnostics. All guidance is based on current UK health policy to ensure accurate and safe information for the public.
