

Jaundice is a medical sign that involves the yellowing of tissues due to high bilirubin levels, but its visual presentation can vary significantly depending on a person’s natural skin colour. While yellowing is the most well known indicator, it is not always easily visible on the surface of the skin. This variation means that healthcare professionals and patients must often look beyond the skin to the whites of the eyes and the mucous membranes to confirm the presence of this condition. Understanding these differences is vital for early detection and ensuring that individuals of all backgrounds receive timely clinical assessment. Because bilirubin can settle in different tissues at different rates, a thorough check of specific areas of the body is necessary to ensure accuracy. This is particularly important in the United Kingdom, where diverse populations require a nuanced approach to physical examinations.
What We’ll Discuss in This Article
- How melanin interacts with bilirubin to affect the visibility of jaundice.
- Why the whites of the eyes are a primary observation site for all ethnicities.
- Key areas to check on darker skin tones, including the mouth and palms.
- The role of lighting and environment in identifying subtle yellowing.
- The biological pathway of bilirubin that remains consistent across all people.
- Non-visual symptoms like dark urine that help confirm a diagnosis.
Visual Variations Based on Skin Pigmentation
Jaundice presents differently on various skin tones because natural melanin can mask the yellow bilirubin pigment on the surface of the skin. In individuals with lighter skin, the yellowing is often quite distinct and can be seen clearly on the face, torso, and eventually the limbs. In contrast, for those with darker skin tones, the yellowing may be subtle, appearing as a dulling of the natural skin tone or being entirely hidden by the concentration of melanin in the epidermis.
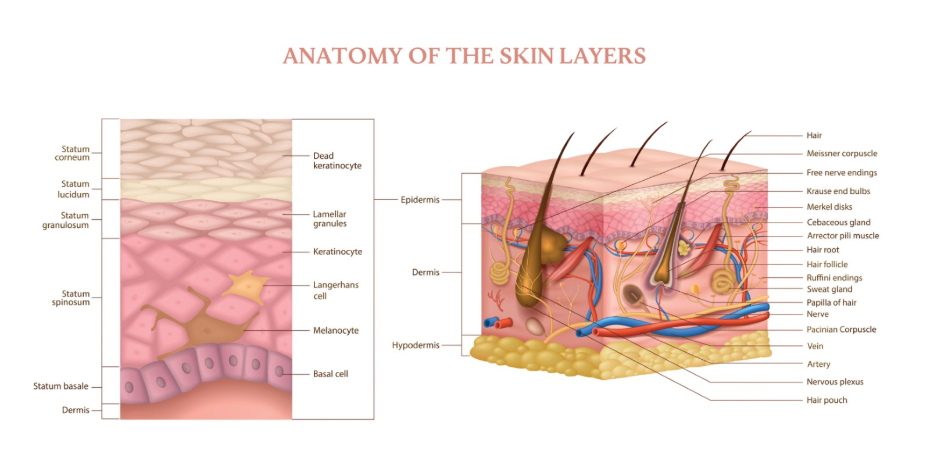
This masking effect occurs because the yellow pigment settles in the dermis and deeper tissues, which are covered by the pigmented outer layers. In the UK, medical training increasingly emphasises the need to look at specific non-pigmented areas to ensure that jaundice is not overlooked in individuals from Black, Asian, and Minority Ethnic backgrounds. Relying solely on a skin colour change can lead to delays in identifying liver or biliary issues, making it essential to understand where else the pigment might be visible.
Primary Sites for Detection on Darker Skin
The whites of the eyes and the mucous membranes are the primary sites for detecting jaundice when it is not visible on the skin surface. The whites of the eyes, known as the sclera, contain high levels of elastin, which has a strong chemical affinity for bilirubin. This means the eyes will often change colour regardless of an individual’s skin tone, making them one of the most reliable indicators for clinical assessment.
In addition to the eyes, healthcare professionals often examine the inside of the mouth, specifically the underside of the tongue and the hard palate on the roof of the mouth. These areas have very little melanin and a rich supply of blood vessels, allowing the yellowing to show through more clearly. The palms of the hands and the soles of the feet may also be checked, as these regions typically have lighter pigmentation and can reveal the yellow hue when other parts of the body do not.
Comparison of Observation Sites Across Skin Tones
Clinical assessments for jaundice must be adapted to account for the natural variations in human pigmentation to ensure accurate results. A systematic approach involves checking several distinct areas to confirm whether bilirubin levels have risen to a point where they are depositing in the tissues.
| Observation Site | Lighter Skin Tones | Darker Skin Tones |
| Face and Torso | Often shows clear yellowing. | Yellowing may be masked or appear as a dullness. |
| Sclera (Eyes) | High visibility of yellow tint. | High visibility; most reliable site. |
| Inside of Mouth | Shows yellowing clearly. | Highly reliable; check hard palate and tongue. |
| Palms and Soles | Shows yellowing clearly. | More reliable than torso or face. |
This comparison highlights why the eyes and mouth are considered universal check points. When a person has a deeper skin tone, the lack of visible yellowing on the arm or chest does not rule out jaundice. Instead, clinicians prioritise the sclera and mucous membranes to provide a more definitive visual assessment.
Biological Mechanisms of Bilirubin Accumulation
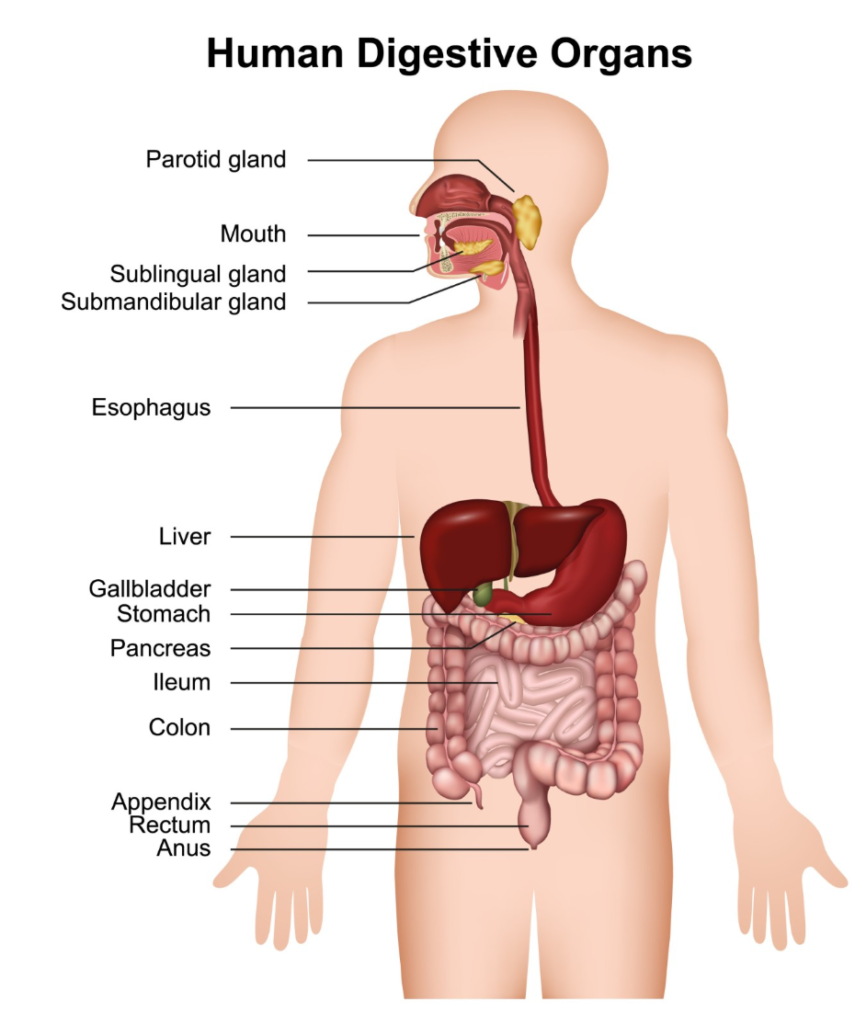
Biological mechanisms of bilirubin accumulation remain the same for all people regardless of their outward appearance or skin tone. Bilirubin is a byproduct of the natural breakdown of old red blood cells, which is a process that occurs continuously in every human body. The NHS explains that jaundice is caused by the build-up of bilirubin in the blood, which happens if the liver is damaged or there is a problem with the bile ducts.
Once produced, bilirubin travels to the liver to be processed and made water soluble so it can be excreted in bile. If this pathway is interrupted, the pigment enters the bloodstream and settles into tissues. Because the affinity of bilirubin for certain proteins like elastin is a chemical property, the internal deposition is identical across all ethnicities. The differences in “look” are purely a result of how much natural skin pigment is layered over the affected tissues, rather than a difference in the underlying medical condition.
The Role of Lighting and Environment in Detection
Optimal lighting is essential for identifying mild or subtle cases of jaundice, especially when the skin tone makes the yellowing difficult to see. Natural daylight is the most effective light source for an accurate examination because it provides a full spectrum of colour, making the yellow tint of bilirubin more apparent. Artificial lighting, particularly warm-toned or yellow-tinted bulbs, can mask the presence of jaundice or create a false impression of yellowing.
In UK clinical settings, healthcare providers are taught to examine patients in “white” light to avoid these visual errors. Patients and carers are also advised to check for changes in the eyes or mouth near a window during the day. For individuals with darker skin, the contrast provided by natural light is even more critical for spotting the faint yellowing of the sclera or the hard palate that might be missed in a dimly lit room.
Identifying Non-Visual Symptoms
Identifying non-visual symptoms is particularly important for patients whose skin tone makes yellowing difficult to see. Because the visual signs can be unreliable, clinicians and patients should monitor for changes in the appearance of bodily waste. NICE guidelines for jaundice in adults state that the presence of dark urine or pale stools can be a significant clinical indicator of a liver or biliary problem even if yellowing is not obvious.
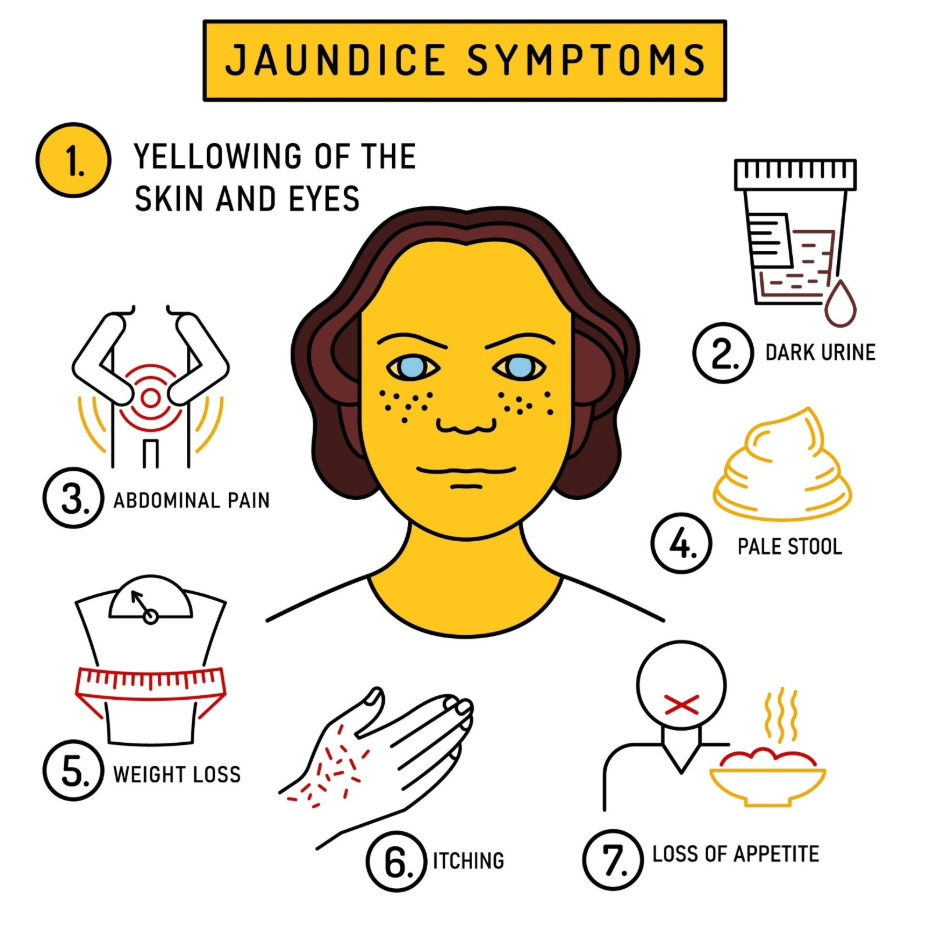
Common non-visual indicators include:
- Dark Urine: Urine that appears a dark orange, brown, or tea colour.
- Pale Stools: Stools that appear clay coloured, grey, or very light.
- Persistent Itching: A sensation of itching that is often worse at night.
- Fatigue: A profound sense of tiredness or general malaise.
- Abdominal Discomfort: Pain or a feeling of heaviness in the upper right side of the stomach.
These symptoms reflect the internal disruption of the biliary system. For example, dark urine occurs when the kidneys try to filter out the excess water-soluble bilirubin that the liver cannot process or the bile ducts cannot drain. These signs are universal and do not depend on skin pigmentation, making them vital tools for a comprehensive health assessment.
Conclusion
Jaundice looks different on various skin tones because melanin can mask the yellowing of the skin, making the examination of the eyes and mouth the most reliable way to detect the condition. While those with lighter skin may show a clear yellow tint on the torso and face, those with darker skin may only show changes in the sclera or the mucous membranes. Non-visual signs like dark urine and pale stools remain consistent across all backgrounds and are crucial for identifying liver or biliary issues. Consistent clinical observation in appropriate lighting is necessary to ensure accuracy. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Why are the whites of the eyes the best place to check for jaundice?
The whites of the eyes contain a protein called elastin which bilirubin binds to easily, and their white background makes the yellow tint highly visible.
Can I have jaundice without my skin turning yellow?
Yes, if you have a darker skin tone, the yellowing may be hidden, or the bilirubin levels may be high enough to affect your eyes but not yet your skin.
Is dark urine always a sign of jaundice?
Dark urine is a common sign of jaundice, but it can also be caused by dehydration or certain medications, so it should always be investigated.
Does the yellowing appear in a specific order?
It often appears first in the eyes and then in the mouth or on the face, eventually spreading to the rest of the body as bilirubin levels rise.
Can certain lights make me look yellow when I am not?
Yes, warm or yellow-tinted artificial lights can make skin and eyes appear yellow, which is why natural daylight is best for an accurate check.
Will jaundice go away on its own?
Jaundice is a symptom of an underlying issue, so the yellowing will usually only fade once the underlying cause is treated.
Are the symptoms different for children and adults?
The visual signs are generally the same, but the underlying causes can differ, so any yellowing in a person of any age needs a medical review.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the presentation of jaundice on various skin tones, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
