

Jaundice can be a significant clinical indicator of pancreatic or bile duct cancer because tumours in these areas often cause a physical obstruction that prevents bile from draining into the digestive tract. When a tumour develops in the head of the pancreas or along the lining of the bile ducts, it can compress or invade the narrow tubes that carry bile from the liver to the intestines. This blockage leads to a buildup of bilirubin in the bloodstream, which then deposits into the skin and the whites of the eyes, resulting in a yellow discoloration. In the United Kingdom, the appearance of jaundice in an adult, particularly if it is not accompanied by pain, is treated as a priority for clinical investigation. While jaundice can be caused by many non-cancerous conditions such as gallstones or hepatitis, healthcare professionals use it as a primary diagnostic marker to rule out more serious structural issues. Understanding the biological connection between biliary drainage and the presence of tumours is essential for ensuring that patients receive timely assessments and appropriate imaging.
What We’ll Discuss in This Article
- The biological mechanism of obstructive jaundice caused by tumours.
- Why pancreatic tumours frequently lead to early yellowing of the skin.
- The specific role of bile duct cancer in interrupting bilirubin excretion.
- Identifying “painless jaundice” as a critical clinical red flag.
- The diagnostic pathway involving blood tests and cross-sectional imaging.
- How the location of a tumour determines the severity of the obstruction.
The Mechanism of Obstructive Jaundice in Cancer
Jaundice linked to pancreatic or bile duct cancer occurs because the tumour creates a mechanical barrier that prevents conjugated bilirubin from leaving the body. The NHS states that jaundice can be a sign of something serious, such as gallstones or a condition affecting the liver or pancreas.
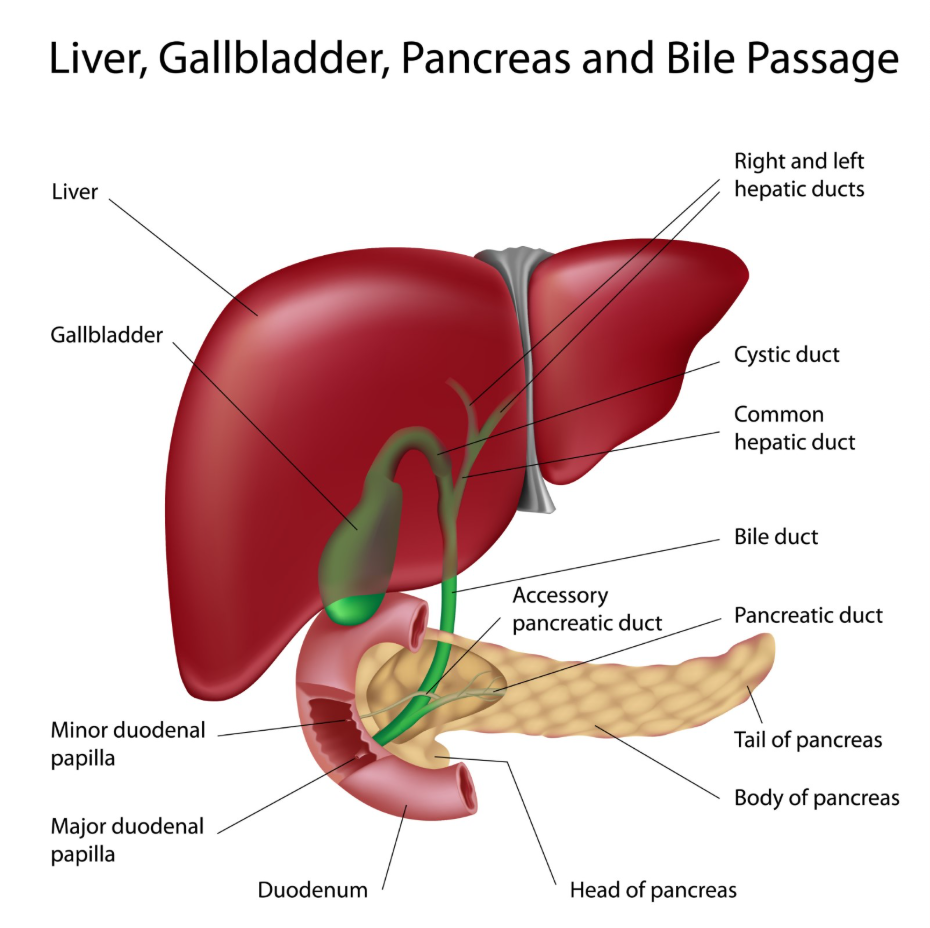
Under normal physiological conditions, the liver processes bilirubin and sends it through the bile ducts into the small intestine. When a tumour grows in the head of the pancreas, it is positioned directly next to the common bile duct. As the tumour expands, it pinches the duct closed. This causes bile to back up into the liver and eventually spill over into the circulatory system. This is classified as post-hepatic or obstructive jaundice. Because the liver has already processed the bilirubin, it is in a water-soluble form that can be filtered by the kidneys, which is why patients with this type of blockage often notice very dark urine.
Pancreatic Cancer and Bile Duct Compression
Pancreatic cancer is one of the most common cancerous causes of jaundice because the majority of these tumours occur in the “head” of the pancreas, which is the part of the organ wrapped around the bile duct. As a tumour grows, it does not have to be very large to exert enough pressure to stop the flow of bile.
In many cases, jaundice is the first visible sign of a problem in the pancreas. Because the blockage develops gradually, the yellowing may appear before the patient feels any significant pain or discomfort. In the United Kingdom, any new onset of jaundice in an adult is investigated with urgency to determine if the pancreas is the source of the obstruction. While other symptoms like weight loss or changes in appetite may occur, the yellowing of the sclera and skin provides the most immediate visual evidence that the biliary drainage system is compromised.
Bile Duct Cancer (Cholangiocarcinoma)
Bile duct cancer, medically known as cholangiocarcinoma, causes jaundice by growing directly within the lining of the tubes that carry bile. These tumours can occur anywhere along the biliary tree, from the small branches inside the liver to the main common bile duct outside the liver.
Because these ducts are quite narrow, even a small growth can lead to a complete obstruction. When the tumour is located at the point where the left and right hepatic ducts meet (known as a Klatskin tumour), it blocks the drainage from both sides of the liver simultaneously. This leads to a rapid rise in bilirubin levels. Jaundice in this context is often accompanied by intense skin itching (pruritus), as bile salts also accumulate in the blood and deposit in the skin alongside the yellow pigment.
Identifying Painless Jaundice as a Red Flag
A critical diagnostic distinction used by UK healthcare professionals is whether the jaundice is “painless” or accompanied by the sharp, cramping pain typical of gallstones. Painless jaundice is considered a high-priority clinical indicator because it is more likely to be associated with a gradual, structural obstruction such as a tumour.
| Feature | Gallstone Obstruction | Cancerous Obstruction |
| Onset of Yellowing | Often sudden | Usually gradual |
| Associated Pain | Often severe (biliary colic) | Often absent or dull ache |
| Weight Loss | Uncommon | Frequently present |
| Stool Colour | May fluctuate | Persistently pale/clay-coloured |
NICE clinical guidelines for suspected cancer in adults highlight that new-onset, unexplained jaundice in individuals over a certain age must be investigated within a two-week urgent pathway. This focus on painless jaundice ensures that structural causes are identified as early as possible, allowing for surgical or medical interventions before the condition progresses further.
Diagnostic Pathways and Investigations
The investigation of jaundice suspected to be linked to cancer follows a structured pathway in the United Kingdom, beginning with biochemical blood tests followed by detailed imaging. Liver Function Tests are used to confirm the obstructive pattern, typically showing very high levels of bilirubin and specific enzymes like Alkaline Phosphatase.
Once a blockage is confirmed by blood work, imaging is required to find the exact cause. An ultrasound scan is often the first step to look for widened ducts or stones. However, if cancer is suspected, more detailed cross-sectional imaging like a CT scan or an MRI is necessary. A specific type of MRI called an MRCP is used to create a detailed three-dimensional map of the bile ducts and pancreas. According to the GOV.UK health pages, timely access to high-quality diagnostic imaging is essential for the early detection and staging of biliary and pancreatic malignancies. These scans allow clinicians to see the size of a tumour and determine if it can be surgically removed or if it is affecting nearby blood vessels.
Management of Jaundice in Cancer Patients
If a tumour is found to be the cause of the jaundice, management focuses on both treating the cancer and relieving the biliary obstruction to improve the patient’s quality of life. High bilirubin levels can cause severe itching, fatigue, and can interfere with the liver’s ability to process chemotherapy.
To relieve the jaundice, a procedure called an ERCP or a PTC may be used to place a stent (a small plastic or metal tube) inside the blocked duct to hold it open. This allows the bile to flow into the intestines again, which leads to the gradual disappearance of the yellowing. Once the jaundice is managed and the liver function improves, the multidisciplinary team can proceed with further treatments such as surgery, chemotherapy, or radiotherapy. Consistent monitoring of bilirubin levels remains an important part of follow-up care for these patients to ensure the stent remains clear and functional.
Conclusion
Jaundice can be linked to pancreatic or bile duct cancer when a tumour physically blocks the drainage of bile, leading to an accumulation of bilirubin in the bloodstream. Painless yellowing of the skin and eyes is a significant clinical marker that requires urgent investigation in the United Kingdom to rule out structural obstructions. Through the use of blood tests and advanced imaging, healthcare professionals can identify the source of the blockage and initiate appropriate management. Early detection is essential for addressing the underlying cause and protecting liver function. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does having jaundice mean I definitely have cancer?
No, jaundice is far more commonly caused by non-cancerous issues like gallstones or hepatitis, but it always needs a medical review to be safe.
Why is “painless” jaundice considered more serious?
Pain often suggests a gallstone moving through the duct, while a lack of pain can suggest a gradual blockage from a growing mass.
Can a tumour be too small to see on a scan?
Very small tumours can sometimes be difficult to see on a standard ultrasound, which is why more detailed CT or MRI scans are used if symptoms persist.
Will the yellowing go away if the tumour is treated?
Yes, if the obstruction is bypassed with a stent or the tumour is surgically removed, the bilirubin levels will drop and the yellowing will fade.
What are “pale stools” and why are they important?
Pale or clay-coloured stools mean bile is not reaching your gut, which is a key sign of a physical blockage in the bile ducts.
Is jaundice always the first symptom of pancreatic cancer?
Not always, but for tumours in the head of the pancreas, it is very often the first visible sign that leads to a diagnosis.
How long does it take to get a scan for jaundice in the UK?
Under the “two-week wait” rule, patients with suspicious jaundice should be seen by a specialist and have initial investigations within 14 days.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the link between jaundice and biliary cancers, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
