

Liver cancer is a significant medical challenge in individuals with advanced cirrhosis because the presence of extensive liver scarring limits the organ’s ability to tolerate aggressive treatments and increases the risk of liver failure. When a primary liver tumour develops within a cirrhotic liver, clinicians must manage two life-threatening conditions simultaneously: the malignancy itself and the underlying loss of liver function. In the United Kingdom, healthcare teams use a structured approach to evaluate the severity of this combination, focusing on how well the remaining healthy liver tissue can support the body while addressing the cancer. Because advanced cirrhosis often means the liver is already struggling to filter toxins and produce essential proteins, the addition of a tumour can lead to a rapid decline in health if not identified early. Understanding the relationship between these two conditions is essential for patients and their families to navigate the complexities of long-term liver care and the available management pathways within the NHS.
What We’ll Discuss in This Article
- The dual burden of managing malignancy and underlying liver scarring.
- How advanced cirrhosis restricts the selection of cancer treatments.
- The clinical impact of reduced liver function on overall stability.
- Why regular surveillance is vital for those with high-level scarring.
- The role of multidisciplinary teams in assessing patient eligibility for care.
- Long-term outcomes and the importance of early-stage detection.
The Dual Clinical Challenge
The seriousness of liver cancer in patients with advanced cirrhosis stems from the fact that the liver is already in a state of chronic dysfunction before the tumour even appears. Primary liver cancer, most commonly hepatocellular carcinoma, usually arises as a direct result of the cellular stress caused by cirrhosis. The NHS states that primary liver cancer is more likely to develop in a liver that has been damaged and scarred over many years, a condition known as cirrhosis.
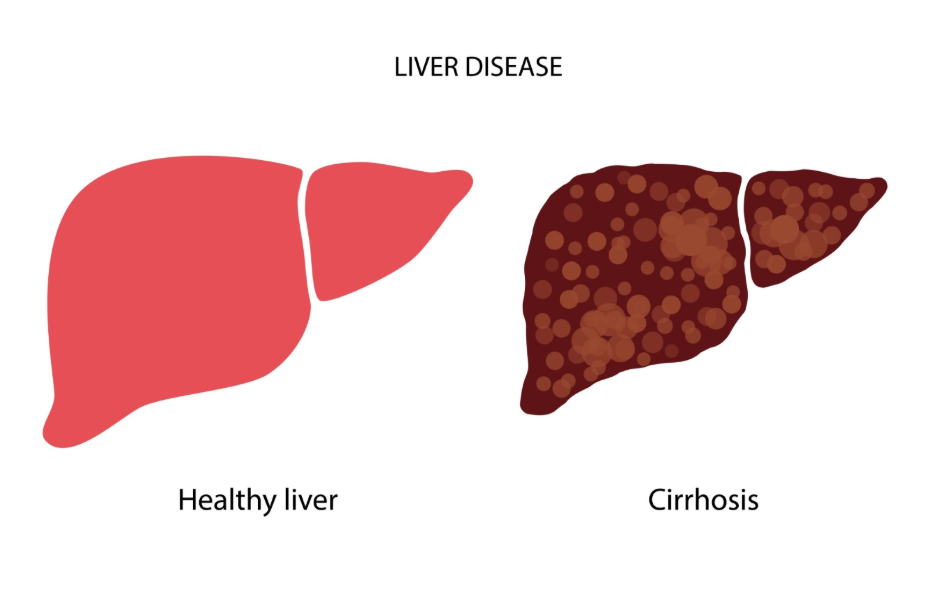
In this scenario, the tumour is not an isolated problem but a complication of a failing organ. The scarring from cirrhosis alters the blood flow through the liver and reduces the number of functional hepatocytes. This means that even a small tumour can have a disproportionate impact on the patient’s health compared to a tumour in a healthy liver. The clinical focus must remain on preserving the fragile balance of liver function while attempting to control the growth of the cancer.
Limitations on Treatment Selection
Advanced cirrhosis often prevents the use of standard cancer treatments like extensive surgery because the liver lacks the regenerative capacity to heal after a portion is removed. In a healthy liver, a surgeon can remove a large tumour, and the remaining tissue will grow back; however, a cirrhotic liver is too stiff and damaged to regenerate effectively. NICE clinical guidelines indicate that the severity of the underlying liver disease is a primary factor in determining whether a patient is suitable for curative treatments such as surgical resection.
| Treatment Type | Suitability in Advanced Cirrhosis | Primary Constraint |
| Surgical Resection | Often Unsuitable | High risk of post-operative liver failure |
| Liver Transplant | Potentially Suitable | Requires meeting strict criteria and donor availability |
| Ablation | Often Suitable | Effective only for small, localised tumours |
| Chemotherapy | Restricted | Liver cannot process many standard drugs safely |
Because the liver processes many medications, the dysfunction caused by advanced cirrhosis also makes certain systemic treatments dangerous. If the liver cannot detoxify the blood, the side effects of cancer drugs can become life-threatening. This necessitates a more conservative approach, often relying on local treatments like heat (ablation) or targeted injections that focus solely on the tumour while sparing the remaining healthy tissue.
Impact on Liver Stability and Decompensation
The presence of liver cancer in a patient with advanced cirrhosis can trigger “decompensation,” where the liver suddenly loses its ability to perform essential tasks. A growing tumour can obstruct the flow of bile or increase the pressure in the portal vein, leading to complications such as jaundice, fluid buildup in the abdomen, or internal bleeding. These events are serious because they indicate that the liver’s functional reserve has been exhausted.
When the liver enters a decompensated state, the patient’s overall health becomes very fragile. The medical team must prioritise stabilising these symptoms, such as using diuretics for fluid or performing procedures to reduce vein pressure, before any cancer-specific management can take place. In many cases, the severity of the cirrhosis itself becomes the limiting factor for life expectancy, regardless of the size or stage of the cancer.
The Role of Surveillance and Early Detection
Because liver cancer is so serious in the context of advanced cirrhosis, the NHS operates a rigorous surveillance programme to find tumours at the earliest possible stage. Individuals with a confirmed diagnosis of cirrhosis are typically offered an ultrasound scan and a blood test every six months. The GOV.UK health pages highlight that regular surveillance is the most effective way to identify liver cancer when it is small enough to be treated despite the presence of cirrhosis.
Finding a tumour while it is less than two or three centimetres in diameter is vital. At this small size, options such as liver transplantation or radiofrequency ablation may still be possible. If a tumour is allowed to grow until it causes symptoms, it is often too late for curative options because the underlying cirrhosis has already compromised the patient’s strength and organ function. Consistent attendance at these six-monthly appointments is the most important factor in managing the severity of this condition.
Multidisciplinary Team Assessment
In the UK, the management of liver cancer in cirrhotic patients is overseen by a multidisciplinary team (MDT) consisting of hepatologists, surgeons, oncologists, and radiologists. This team uses a grading system to assess both the stage of the cancer and the severity of the cirrhosis. This comprehensive evaluation ensures that the risks of any intervention are carefully weighed against the potential benefits for the patient’s specific liver health.
The MDT looks at factors such as the patient’s level of bilirubin, albumin, and blood clotting ability to determine the liver’s “functional score.” If the score suggests the liver is too weak, the team will focus on supportive care and symptom management to maintain quality of life. This personalised approach is essential because every patient with advanced cirrhosis has a unique level of organ damage, and a “one size fits all” treatment plan would be clinically unsafe.
Conclusion
Liver cancer is a very serious condition in people with advanced cirrhosis because it further compromises an already failing organ and limits the available medical options. The severity is determined by the balance between the tumour’s growth and the liver’s remaining functional capacity. Early detection through regular NHS surveillance remains the best strategy for identifying manageable tumours before the liver becomes too weak to tolerate care. Proactive management by a specialist team is essential for navigating the complex relationship between these two chronic conditions. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can liver cancer be cured if I have cirrhosis?
It can be cured or managed for a long time if found very early, often through a liver transplant or small-scale ablation.
Why can’t I have normal chemotherapy for liver cancer?
Standard chemotherapy is often too toxic for a cirrhotic liver to process, so specialists prefer treatments that target only the tumour.
Does cirrhosis always turn into liver cancer?
No, while the risk is much higher, many people live with cirrhosis for years without ever developing cancer.
What is the first sign that cancer is developing in a scarred liver?
There is often no first sign, which is why ultrasound scans are used to find tumours before they cause symptoms.
Can a liver transplant fix both the cirrhosis and the cancer?
Yes, for patients who meet specific criteria, a transplant replaces the scarred liver and removes the cancer at the same time.
What happens if my liver is too weak for cancer treatment?
If the cirrhosis is very advanced, the medical team will focus on “palliative” care, which means managing pain and keeping you comfortable.
How long can someone live with both conditions?
This varies greatly depending on how early the cancer is caught and how well the liver is functioning; some people remain stable for several years with the right care.
Authority Snapshot (E-E-A-T)
This article provides medically factual health information regarding the severity of liver cancer in cirrhotic patients, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in internal medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
