

A liver transplant is considered the only definitive cure for end-stage cirrhosis, but it is not the only management option for individuals living with advanced liver scarring. In the United Kingdom, medical care for end-stage liver disease focuses on a dual approach: managing the life-threatening complications of the condition while simultaneously assessing whether a patient is a suitable candidate for a transplant. For some patients, a transplant may be unsuitable due to other underlying health conditions or personal circumstances, shifting the clinical focus toward palliative or supportive care aimed at maintaining comfort and quality of life. The liver is a vital organ responsible for over 500 functions, and when it reaches the stage of end-stage failure, it can no longer support the body’s basic metabolic and filtration needs. Navigating these options requires a comprehensive evaluation by a specialist multidisciplinary team to determine the safest and most appropriate pathway for each individual. Understanding the breadth of supportive treatments available alongside transplantation helps patients and families make informed decisions about long-term liver care.
What We’ll Discuss in This Article
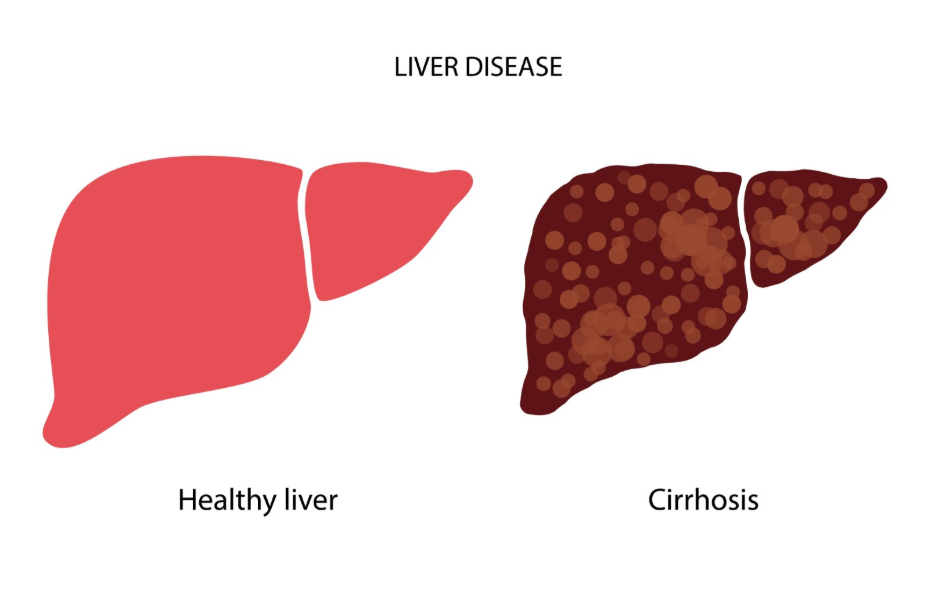
- The definition of end-stage cirrhosis and its impact on organ function.
- How a liver transplant serves as a definitive replacement for a failing organ.
- Medical management of complications such as ascites and hepatic encephalopathy.
- The role of supportive and palliative care for patients unsuitable for transplant.
- Criteria used in the UK to determine eligibility for a liver transplant.
- Lifestyle and nutritional support as part of a holistic management plan.
The Role of Liver Transplantation in Advanced Disease
A liver transplant is the most effective treatment for end-stage cirrhosis because it involves physically replacing the scarred and failing organ with a healthy liver from a donor. This procedure is generally reserved for patients whose liver function has deteriorated to a point where it is no longer life-sustaining or for those who have developed liver cancer within specific criteria. The NHS states that a liver transplant may be an option for people with liver failure or liver cancer when other treatments are no longer working.
In the UK, the success of a transplant relies on careful patient selection and life-long follow-up care. While a transplant can restore normal liver function, it is a major surgical undertaking that requires the patient to be physically strong enough to survive the operation and the subsequent recovery process. Because the demand for donor livers exceeds the supply, the NHS uses a rigorous scoring system to ensure that those with the greatest clinical need are prioritised on the waiting list.
Managing Complications Without Surgery
Medical treatments are used to manage the symptoms of end-stage cirrhosis and maintain stability, even when a transplant is not immediately possible or appropriate. These treatments focus on controlling the side effects of liver failure, such as the buildup of fluid in the abdomen (ascites) or the accumulation of toxins in the blood that can affect brain function. Diuretics and low-sodium diets are standard interventions to help the body process excess fluid.
For patients at risk of internal bleeding from enlarged veins in the food pipe, medications like beta-blockers or procedural interventions such as endoscopic banding are used. While these treatments do not fix the underlying scar tissue, they are vital for preventing emergency hospitalisations and preserving the patient’s current health status. NICE clinical guidelines indicate that the effective management of portal hypertension and its complications is a critical component of care for all patients with advanced cirrhosis.
Supportive and Palliative Care Pathways
Supportive and palliative care is a significant treatment option for patients with end-stage cirrhosis who are either not eligible for a transplant or choose not to pursue one. This pathway focuses on the relief of symptoms and the improvement of quality of life rather than curing the underlying disease. It involves a team of specialists who address physical pain, nutritional needs, and psychological well-being.
| Care Aspect | Clinical Focus | Common Interventions |
| Symptom Control | Managing pain and itching | Specific medications and skin care. |
| Fluid Management | Reducing abdominal swelling | Paracentesis (fluid drainage) and diet. |
| Mental Clarity | Managing confusion | Lactulose or Rifaximin to lower toxins. |
| Nutrition | Preventing muscle wasting | High-protein snacks and calorie support. |
Palliative care is not just for the very end of life; it is an integrated approach that can be provided alongside other medical treatments. In the UK, this ensures that patients who cannot undergo a transplant still receive comprehensive medical oversight. The goal is to ensure the patient remains as comfortable and independent as possible, with their dignity and personal preferences at the centre of the care plan.
Eligibility Criteria for UK Transplant Assessment
Determining if a transplant is the right option involves a complex assessment that evaluates the patient’s overall fitness and the likelihood of a successful outcome. Not every patient with end-stage cirrhosis is a candidate for surgery. Specialists must consider the health of the heart, lungs, and kidneys, as well as the presence of any other active infections or malignancies outside the liver.
The GOV.UK health pages indicate that the assessment for a liver transplant is a thorough process that looks at the patient’s physical and psychological readiness for life-long immunosuppression. Patients must also show a commitment to total abstinence if their liver disease was caused or worsened by alcohol. This ensures that the limited resource of donor organs is used where it provides the greatest long-term survival benefit. If a patient is deemed unsuitable, the clinical team will transition them to the most effective supportive care pathway.
Holistic Support and Nutritional Management
Nutritional and holistic support is an essential treatment pillar for all patients with end-stage cirrhosis, regardless of their transplant status. Because the liver is responsible for processing nutrients, advanced scarring often leads to severe malnutrition and muscle wasting. Providing the body with adequate energy and protein is necessary to prevent infections and maintain the strength needed for daily activities.
Dietitians within the NHS work with patients to create high-calorie, high-protein eating plans that avoid excess salt. This often includes small, frequent meals throughout the day and a complex carbohydrate snack before bed to prevent the body from entering a fasting state overnight. Maintaining muscle mass is not just about physical strength; it also helps the body process certain toxins, which can reduce the severity of brain fog associated with liver failure.
Conclusion
While a liver transplant is the only definitive cure for end-stage cirrhosis, medical management of complications and supportive palliative care are essential treatment options for maintaining stability and quality of life. The choice of pathway depends on a thorough clinical assessment of the patient’s overall health and the functional capacity of their remaining liver tissue. For those unsuitable for surgery, the UK health system provides robust symptom management focused on comfort and dignity. Adhering to specialist advice regarding nutrition and medication remains vital for all patients living with advanced liver scarring. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is it ever too late for a liver transplant?
A transplant may be considered too high risk if the patient’s other organs are failing or if they are too physically weak to survive the major surgery.
What happens if I am not eligible for a transplant?
The medical team will focus on supportive care to manage your symptoms, keep you comfortable, and prevent complications like fluid buildup.
Can I live a long time without a transplant?
With careful medical management of symptoms and a strict diet, some people can remain stable in a compensated state for a significant period.
How long is the wait for a liver transplant in the UK?
The wait time varies depending on your blood group, size, and clinical urgency, with some patients waiting days and others waiting many months.
Why do I need to stop drinking to get a transplant?
Total abstinence is required to ensure the new liver is not damaged and to confirm the patient is committed to long-term organ health.
Is paracentesis a cure for liver fluid?
No, it is a procedure to drain the fluid to make the patient more comfortable, but the fluid will likely return unless the liver function improves.
Does a transplant fix everything?
A transplant replaces the liver, but patients must take anti-rejection medication for the rest of their lives and attend regular follow-up appointments.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding end-stage cirrhosis management, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general surgery, internal medicine, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
