

A family history of colon polyps does not directly increase the biological risk of developing diverticulitis, as these two conditions arise from different pathological processes within the large intestine. While colon polyps involve the overgrowth of cells on the inner lining of the bowel, diverticulitis is an inflammatory condition affecting small, outward-bulging pouches in the colon wall known as diverticula. Although there is no direct causal link between the genetic predisposition for polyps and the structural development of diverticular disease, both conditions are highly prevalent in the United Kingdom and share several non-genetic risk factors such as age and long-term dietary habits. In the UK healthcare system, clinicians manage these issues as separate medical entities, though they are frequently identified together during diagnostic investigations like a colonoscopy. Understanding that the genetic mechanisms driving cellular mutations in polyps are distinct from the mechanical factors causing diverticula is essential for patients navigating their gastrointestinal health. By identifying individual risk factors for both conditions, healthcare providers can ensure that patients receive the appropriate preventative screening for polyps while managing the dietary and lifestyle needs associated with diverticular health.
What We’ll Discuss in This Article
- The distinct biological origins of polyps and diverticula.
- How family history specifically impacts the risk of colon polyps.
- The role of genetics versus lifestyle in the development of diverticulitis.
- Why both conditions are frequently found in the same family groups.
- Shared environmental and dietary factors that affect bowel health.
- UK clinical guidelines for screening and managing multiple bowel risks.
Distinct Biological Origins of Polyps and Diverticulitis
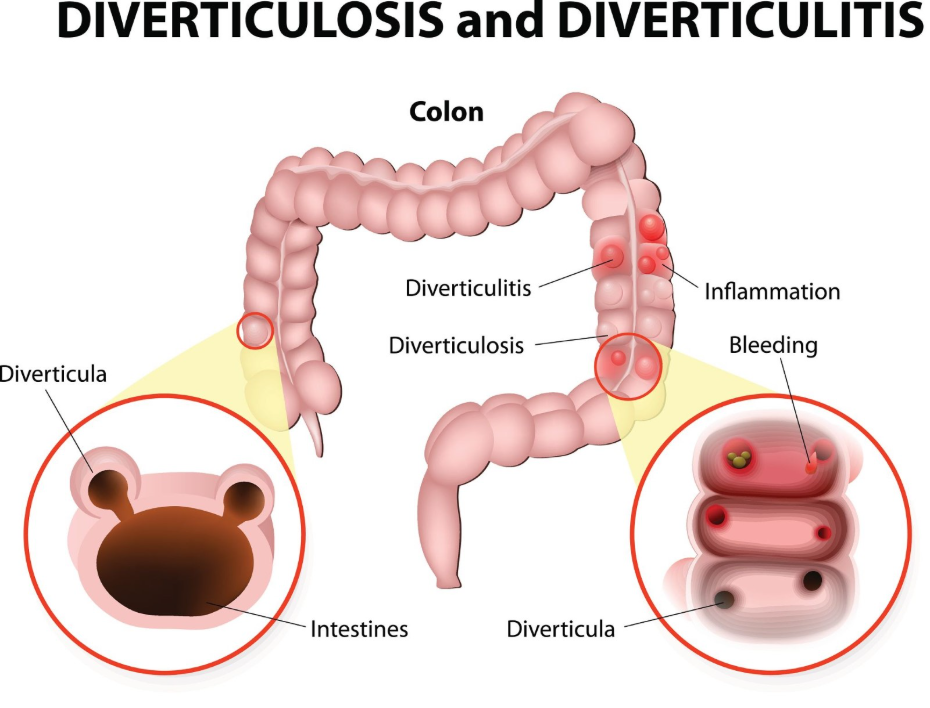
The primary reason a family history of polyps does not translate to an increased risk of diverticulitis is that the conditions involve different layers and orientations of the bowel wall. A colon polyp is a clump of cells that grows on the mucosa, the innermost lining of the colon, and extends inward into the space where waste passes.
In contrast, diverticulitis involves diverticula, which are small pockets created when the inner lining pushes out through weakened areas in the outer muscular layer of the bowel. The NHS states that bowel polyps are small growths on the inner lining of the large intestine, whereas diverticular disease and diverticulitis are related to small bulges in the lining of the large intestine. Because polyps are a failure of regulated cell division and diverticula are a failure of the muscular wall’s integrity under pressure, the genetic instructions for one do not typically influence the other.
How Family History Impacts Colon Polyp Risk
A family history of polyps is a significant clinical indicator for an increased risk of developing similar growths, as certain genetic mutations that control cell renewal can be inherited. If a close relative has had adenomatous polyps, an individual may be more likely to develop them because they have inherited a predisposition for faster cell division in the bowel lining.
NICE clinical guidelines for colorectal cancer prevention emphasise that individuals with a strong family history of polyps or bowel cancer should be offered earlier or more frequent screening to identify and remove growths. These genetic factors are specific to the “on” and “off” switches of cell growth. While these mutations increase the probability of polyps, they do not affect the strength of the colon’s muscular wall or the internal pressure that leads to the formation of diverticula.
Genetics versus Lifestyle in Diverticulitis
While there is some evidence that a family history of diverticulitis may increase an individual’s risk, this is generally thought to be linked to shared dietary habits and inherited connective tissue strength rather than a link to polyps. Diverticulitis occurs when diverticula become inflamed or infected, often due to high internal pressure from constipation or low-fibre intake.
In the United Kingdom, diverticular disease is very common in older age, and family members often share the same Western-style diets that are low in fibre and high in processed foods. NICE clinical guidelines for diverticular disease management identify a low-fibre diet as a major modifiable risk factor for the development of diverticula and subsequent flare-ups of diverticulitis. Therefore, if multiple family members have diverticulitis, it is often more a reflection of shared lifestyle and environment than a genetic link to cellular overgrowths like polyps.
Shared Risk Factors for Bowel Conditions
The reason polyps and diverticulitis are often found in the same families is due to shared non-genetic risk factors that impact the health of the entire colon simultaneously. Both conditions become significantly more common as individuals age and are influenced by long-term metabolic health.
| Factor | Impact on Polyps | Impact on Diverticulitis |
| Low Fibre Intake | Increases contact time for toxins in the bowel. | Increases internal pressure and constipation. |
| High Red Meat Diet | Linked to DNA damage in the bowel lining. | Often associated with a low-fibre, high-fat diet. |
| Obesity | Associated with metabolic stress and cell growth. | Linked to higher systemic inflammation. |
| Sedentary Lifestyle | May slow bowel transit and influence cell health. | Can lead to slower waste passage and pressure. |
In the UK, public health initiatives such as the national bowel screening programme and nutritional guidance address these shared risks. By managing weight and increasing fibre, family members can reduce their independent risks for both conditions, even if they have a genetic predisposition for one of them.
Clinical Screening and Diagnostic Pathways
In the United Kingdom, clinical investigations are tailored to the specific risk profile of the patient, ensuring that a family history of polyps triggers the correct preventative screening without assuming an increased risk for diverticular issues. If a patient reports a family history of polyps, they may be entered into a surveillance programme earlier than the standard national screening age.
During a colonoscopy, the endoscopist will inspect the entire lining of the large intestine. While they may find diverticula during this process, the presence of diverticula is usually noted as an incidental structural finding. The GOV.UK health pages indicate that the primary goal of the bowel screening programme is the early detection and removal of polyps to prevent more serious conditions. If a patient has symptoms of diverticulitis, such as lower left abdominal pain, a CT scan is often used for diagnosis rather than relying on a family history of polyps.
Managing Multiple Bowel Risks in the UK
Management of bowel health for individuals with a family history of polyps involves a dual approach: vigilant screening for cellular growths and proactive lifestyle management to protect the structural integrity of the colon. Patients are often advised that while they cannot change their genetics, they can influence the environment of their colon through diet and hydration.
Consistent follow-up is necessary for those who have had polyps removed to ensure that new growths are identified promptly. Simultaneously, maintaining soft, bulky stools through high fibre intake protects the colon from the high pressures that cause diverticula. This comprehensive care pathway ensures that the UK population is protected from both the slow cellular changes of polyps and the acute inflammatory risks of diverticulitis. By understanding that these are separate risks, patients can work with their healthcare teams to ensure every aspect of their bowel health is monitored and supported effectively.
Conclusion
A family history of polyps does not increase the risk of diverticulitis, as the two conditions have distinct biological causes and affect different structures of the bowel. While polyps are driven by genetic mutations in cell growth, diverticulitis is largely influenced by age, bowel pressure, and dietary habits. In the UK, these conditions are managed through separate screening and treatment pathways to ensure comprehensive care. Maintaining a healthy lifestyle and participating in all offered screenings are the most effective ways to manage the health of the colon wall and lining. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
If my parents had polyps, do I need to worry about diverticulitis?
Not directly; having a family history of polyps means you should be vigilant about bowel screening, but diverticulitis risk is more closely linked to your own diet and lifestyle.
Can a polyp turn into a diverticulum?
No, they are two different structural issues; a polyp is an inward growth of tissue, while a diverticulum is an outward bulge in the wall.
Why did my doctor find both diverticula and polyps during my check-up?
It is very common for both to be found together in adults in the UK because they both become more likely as you get older.
Is the screening for polyps the same as the test for diverticulitis?
No; polyps are usually found through stool tests or colonoscopy screening, while diverticulitis is typically diagnosed during an acute flare-up using a clinical exam or CT scan.
Does a high-fibre diet prevent both polyps and diverticulitis?
A high-fibre diet is the standard UK recommendation for general bowel health, as it supports a healthy lining and reduces pressure in the colon.
Can diverticulitis make it harder to find polyps in my family members?
If a family member has severe diverticular disease, the pouches can sometimes make it more challenging to see every part of the bowel lining, but UK clinicians are trained to manage this.
Does diverticulitis run in families like polyps do?
While there may be some inherited factors in tissue strength, diverticulitis is much less “genetic” than certain types of polyps and is heavily influenced by shared family diets.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the relationship between a family history of polyps and diverticulitis risk, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine, general surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.
