

Some people have polyps without symptoms because these growths are typically small, slow-growing clusters of cells that do not irritate the bowel wall, whereas diverticulitis involves an acute infection or inflammation that triggers the body’s pain response. Colon polyps are protrusions on the inner lining of the large intestine that often exist for years without disrupting the passage of waste or causing physical discomfort. In contrast, diverticulitis occurs when small pouches in the colon wall become blocked or infected, leading to localised swelling, pressure, and systemic signs of illness. In the United Kingdom, healthcare professionals distinguish between these two conditions based on their physiological impact: one is a silent structural change, while the other is an active inflammatory event. Because polyps are frequently asymptomatic, they are usually detected through routine screening programmes designed to find them before they progress. Diverticulitis, however, is often identified when a patient seeks medical help for sudden abdominal pain or fever. Understanding these biological differences is essential for recognising why some bowel conditions require proactive screening while others present with clear clinical warning signs.
What We’ll Discuss in This Article
- The biological reasons why colon polyps are typically asymptomatic.
- How the inflammatory process in diverticulitis triggers severe pain.
- Structural differences between inward-growing polyps and outward-bulging pouches.
- The role of the nervous system in detecting bowel inflammation versus growths.
- Why regular screening is necessary for “silent” bowel conditions.
- UK clinical pathways for managing both asymptomatic and symptomatic findings.
The Asymptomatic Nature of Colon Polyps
Colon polyps are generally asymptomatic because they grow very slowly on the inner mucosal lining and do not possess the infectious or inflammatory triggers that cause pain. A polyp is a clump of surplus cells that forms when the normal cycle of cell renewal in the colon is disrupted. The NHS states that bowel polyps are common and usually do not cause symptoms, though some can cause rectal bleeding or a change in bowel habits.
Most polyps are small and do not interfere with the movement of waste through the large intestine. Because the inner lining of the colon does not have the same concentration of sensory nerves for “touch” as the skin, a small growth can exist for a long time without the individual feeling its presence. It is only when a polyp becomes exceptionally large that it might cause a partial obstruction or bleed due to mechanical friction from passing waste. In the United Kingdom, the healthcare system relies on biochemical tests and visual inspections, such as colonoscopies, to find these silent growths. This proactive approach is necessary because relying on physical symptoms for polyp detection would result in many growths going unnoticed for decades.
Why Diverticulitis Triggers Acute Physical Signs
Diverticulitis causes serious physical signs because it involves an active bacterial infection or a tear in the bowel wall that stimulates the body’s acute inflammatory response. Diverticula are small pockets that push out through weakened areas of the colon’s muscular layer, a condition known as diverticulosis. While diverticulosis itself is often as silent as a polyp, diverticulitis occurs when one of these pockets becomes blocked by waste or sustains a micro-perforation. The NHS explains that diverticulitis happens when pouches in the large intestine become inflamed or infected, leading to severe abdominal pain and fever.
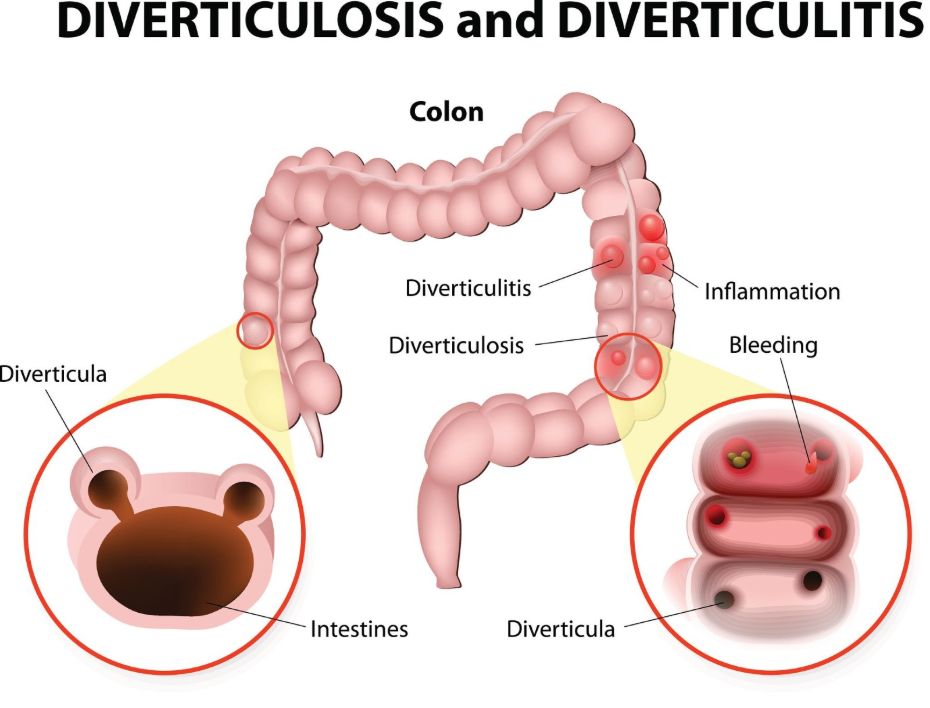
When bacteria multiply within a trapped pouch, the tissue becomes swollen, red, and tender. This inflammation irritates the peritoneum, which is the sensitive lining of the abdominal cavity. The nervous system reacts to this irritation by sending sharp pain signals to the brain, usually localised to the lower left side of the abdomen. Additionally, the body responds to the infection by raising the internal temperature, resulting in a fever. These “serious signs” are the body’s way of indicating that the integrity of the bowel wall is under threat and requires medical assessment to prevent complications such as an abscess or perforation.
Comparing Inward Growths and Outward Pouches
The structural orientation of polyps and diverticula influences how they interact with the colon and why their symptom profiles are so different. Polyps grow inward from the mucosa into the lumen, the space where waste travels, whereas diverticula are protrusions that bulge outward away from the lumen.
| Feature | Colon Polyps | Diverticulitis |
| Growth Direction | Inward (into the colon). | Outward (away from the colon). |
| Tissue Impact | Localised cellular overgrowth. | Full-thickness wall inflammation. |
| Nerve Involvement | Minimal irritation to sensory nerves. | High irritation of abdominal lining. |
| Typical Onset | Very slow (years). | Acute (hours or days). |
| Primary Danger | Potential for cellular changes. | Potential for infection or burst pouch. |
Because polyps only involve the superficial layers of the bowel lining, they rarely cause the systemic distress seen in diverticulitis. Diverticulitis involves the entire thickness of the bowel wall and can affect the space outside the colon, leading to the sharp, constant pain that patients report. In the UK, clinicians use these structural differences to determine which diagnostic tool is most appropriate; a colonoscopy is ideal for seeing polyps inside the bowel, while a CT scan is often preferred for assessing the outward inflammation and complications of diverticulitis.
Sensory Nerves and the Detection of Bowel Issues
The human colon has different types of sensory receptors, and diverticulitis triggers the nerves that detect stretching and inflammation, which polyps typically do not affect. The visceral nerves in the gut are highly sensitive to “distension” (stretching) and “ischaemia” (lack of blood flow), both of which occur during a diverticulitis flare-up as the pouch swells and the surrounding tissue becomes inflamed.
NICE clinical guidelines for diverticular disease management highlight that constant, severe abdominal pain is a hallmark of acute diverticulitis because of how the inflammation affects the surrounding nerves and abdominal lining. Polyps, unless they grow large enough to cause a total blockage, do not cause the bowel wall to stretch or lose its blood supply in the same way. Consequently, the brain does not receive pain messages from a polyp. This biological discrepancy is why an individual can feel perfectly healthy while harbouring several polyps, yet feel profoundly ill during an episode of diverticulitis. Understanding this nerve response helps explain why the absence of pain is not a guarantee of a clear colon.
The Necessity of Proactive Screening for Silent Growths
Because polyps are silent, the UK national bowel screening programme is designed to detect them using biochemical markers like hidden blood, rather than waiting for physical symptoms to appear. The Faecal Immunochemical Test (FIT) used in the UK looks for microscopic amounts of blood that can be shed by polyps as waste passes over them.
If the test is abnormal, it indicates that a growth may be present, even if the person has no pain or habit changes. This screening is vital because it identifies polyps when they are small and most easily removed during a colonoscopy. Diverticulitis does not have a similar national screening programme because its symptoms pain and fever usually prompt the patient to seek care when an episode occurs. By participating in offered screenings, individuals can ensure that “silent” conditions are managed just as effectively as those that cause obvious distress. This dual approach of symptom-led care for diverticulitis and screening-led care for polyps ensures the best outcomes for long-term bowel health.
UK Clinical Pathways for Bowel Investigations
In the United Kingdom, healthcare providers use integrated pathways to investigate both symptomatic and asymptomatic bowel findings, ensuring that all structural changes are accounted for. If a patient presents with the serious signs of diverticulitis, the immediate focus is on resolving the infection and inflammation.
Once the acute episode has subsided, a follow-up colonoscopy may be performed to ensure the bowel is healthy and to check for any hidden polyps. This is important because the symptoms of diverticulitis can occasionally mask the presence of polyps in the same area. Standard UK practice involves treating the acute inflammatory issue first before proceeding with preventative cancer screening. Following this structured pathway allows clinicians to provide comprehensive care that addresses both the immediate crisis of an infection and the long-term risk of cellular overgrowth. By managing both the “silent” and the “loud” conditions, the UK healthcare system maintains the functional and structural stability of the colon throughout the patient’s life.
Conclusion
Polyps are often silent because they are slow-growing tissue clusters that do not cause inflammation, whereas diverticulitis presents with serious signs due to acute infection and nerve irritation. While the absence of symptoms is common with polyps, it does not mean the colon is clear, which is why UK national screening is essential. Diverticulitis, with its characteristic pain and fever, requires prompt medical assessment to manage the active inflammatory process. Understanding these different clinical presentations ensures that individuals participate in preventative checks while also seeking timely help for acute symptoms. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a polyp eventually cause pain like diverticulitis?
Only if it grows large enough to cause a complete bowel obstruction, which is rare as most are found and removed during screening first.
Why does diverticulitis make me feel so much more ill than polyps?
Diverticulitis is an active infection that triggers a whole-body immune response, including fever, while polyps are just extra tissue.
If I have diverticula, am I more likely to have polyps?
Not necessarily; while both are common as people get older in the UK, they are caused by different biological processes.
Can a home screening kit find diverticulitis?
No, the kit looks for microscopic blood often associated with polyps; diverticulitis is usually diagnosed by a doctor based on your physical symptoms.
Will my polyps hurt if my diverticulitis flares up?
No, polyps do not have the nerves to feel pain, but the general inflammation in your bowel from diverticulitis will cause widespread discomfort.
Does a healthy diet prevent both conditions?
A high-fibre diet is the standard UK recommendation for general bowel health as it supports a healthy lining and reduces pressure in the colon.
What is the most reliable way to find silent polyps?
A colonoscopy is the most reliable method as it allows a clinician to see the entire inner lining of the bowel and remove any growths found.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the differences between colon polyps and diverticulitis symptoms, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine, general surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.