

A colonoscopy is a highly effective diagnostic procedure that can detect both colon polyps and the structural presence of diverticulitis simultaneously by providing a direct high-definition view of the entire inner lining of the large intestine. During the examination, a clinician uses a thin, flexible tube equipped with a camera to identify various abnormalities, including tissue growths that protrude into the bowel lumen and small pouches that bulge outward from the colon wall. While polyps and diverticula are distinct conditions involving different biological processes, they are frequently discovered together because they share common risk factors like age and long-term dietary patterns. In the United Kingdom, healthcare professionals utilise colonoscopies as the primary tool for both colorectal cancer screening and the investigation of symptomatic bowel disease. Identifying these conditions at the same time allows for a comprehensive assessment of a patient’s gastrointestinal health, ensuring that preventative measures and management strategies are aligned. Understanding how a single procedure can address multiple bowel concerns is essential for patients undergoing diagnostic reviews or participating in national screening programmes. By providing a clear visual map of the colon, the UK healthcare system can effectively manage the separate risks associated with cellular overgrowths and structural wall changes.
What We’ll Discuss in This Article
- How the colonoscopy procedure visualises both inward and outward bowel changes.
- The difference between detecting polyps and identifying diverticular disease.
- Why clinicians avoid performing colonoscopies during active inflammatory flare-ups.
- The clinical benefits of identifying multiple bowel conditions in a single session.
- How a colonoscopy allows for the immediate removal of detected polyps.
- UK clinical protocols for follow-up care when both conditions are present.
Visualising Polyps and Diverticula During the Procedure
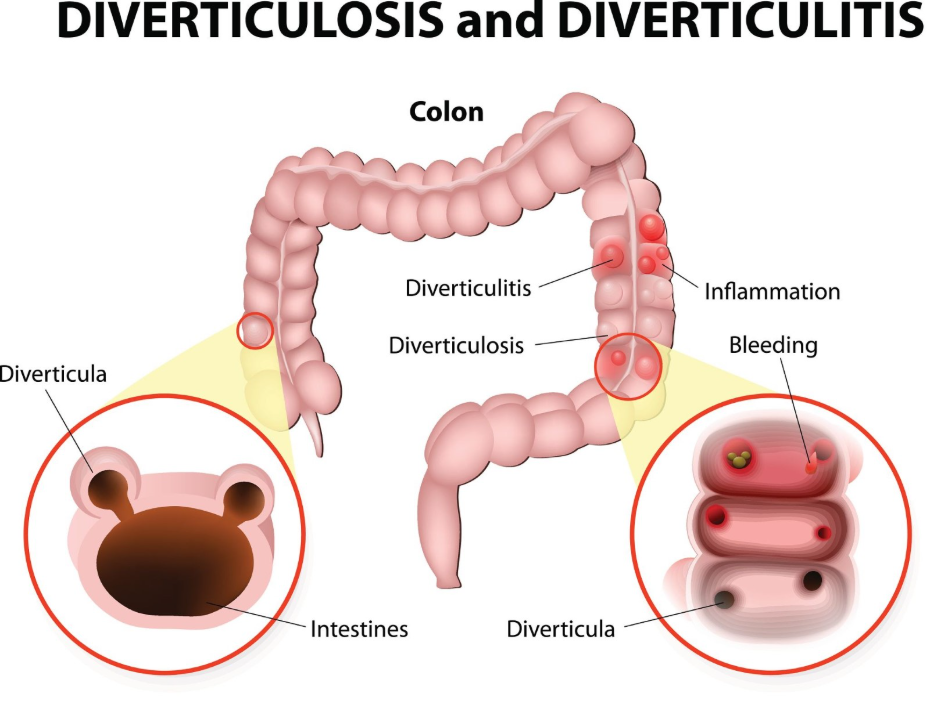
A colonoscopy detects both polyps and diverticula by allowing the clinician to inspect every centimetre of the mucosal lining for protrusions and indentations while the bowel is gently inflated with air. As the camera moves through the large intestine, it can easily distinguish between a polyp, which is an extra clump of tissue growing into the space where waste passes, and diverticula, which appear as small openings or “pockets” in the bowel wall. The NHS states that a colonoscopy is a procedure to look inside your bowels and can find things like small growths called polyps or small bulges called diverticula.
The direct visual nature of the test ensures that even small abnormalities can be mapped and recorded. In many cases, these conditions are found in the same areas of the colon, particularly the sigmoid colon on the lower left side, where internal pressure is often highest. Because the clinician can see the texture and colour of the lining in real-time, they can also assess if there are any signs of chronic inflammation or irritation. In the United Kingdom, this dual detection capability makes the colonoscopy the most thorough investigation for patients presenting with non-specific bowel symptoms or those reaching the age threshold for national screening.
Distinguishing Between Polyps and Diverticular Disease
While a colonoscopy can identify both conditions at once, it is important to understand that they represent different types of structural change with distinct clinical implications. A polyp is a cellular overgrowth on the inner lining that is monitored because some types, known as adenomas, may progress toward more serious conditions over several years. Diverticulitis, however, is a condition where small pouches (diverticula) have formed in the colon wall and subsequently become inflamed or infected.
| Feature | Colon Polyps | Diverticular Disease |
| Visual Appearance | Fleshy bumps or mushroom-like growths. | Small, dark pits or pocket openings. |
| Orientation | Protrudes into the bowel lumen. | Bulges outward from the bowel wall. |
| Action Taken | Typically removed during the procedure. | Noted and managed with dietary advice. |
| Primary Goal | Cancer prevention and tissue analysis. | Symptom management and risk reduction. |
During the procedure, the endoscopist will prioritise the removal of any polyps they find, a process called a polypectomy. Diverticula cannot be removed in the same way, as they involve the full thickness of the bowel wall; instead, their presence is documented to help guide the patient’s long-term dietary and lifestyle management. In the UK, the discovery of both conditions is a common clinical finding that helps healthcare providers provide a personalised care plan addressing both cellular and structural health.
Timing and Safety During Active Inflammation
Although a colonoscopy is effective for detecting diverticula, it is generally postponed if a patient is experiencing an active flare-up of diverticulitis due to the increased risk of bowel perforation. When diverticula become acutely infected or inflamed, the bowel wall becomes fragile and swollen. NICE clinical guidelines for diverticular disease management indicate that a colonoscopy or other invasive bowel tests should usually be delayed until the acute inflammation has resolved, typically after 6 to 8 weeks.
Performing the procedure during a flare-up could cause a weakened pouch to burst under the pressure of the air used to inflate the colon. Instead, UK clinicians often use a CT scan to diagnose the infection during the acute phase. Once the inflammation has settled and the tissue has healed, a follow-up colonoscopy is then scheduled. This delay ensures that the clinician can safely and clearly inspect the bowel lining to check for polyps that might have been obscured by the previous swelling, ensuring a comprehensive and safe diagnostic result.
Immediate Intervention: Polypectomy During Detection
One of the significant advantages of detecting both conditions during a colonoscopy is the ability to remove polyps immediately, thereby reducing future risks while the diverticula are being assessed. If a clinician identifies a polyp, they can pass specialised tools through the colonoscope to snip it off or use a wire loop to remove it. This prevents the need for a separate procedure and provides immediate preventative care.
The presence of diverticula does not typically prevent the removal of polyps, although the endoscopist must navigate carefully if the bowel is particularly distorted by diverticular disease. After the polyp is removed, it is sent to a laboratory to determine its specific type and to see if there are any cellular changes. In the United Kingdom, this integrated approach to detection and treatment is a cornerstone of gastrointestinal health, allowing patients to leave the procedure with their cancer risk reduced and a clear understanding of their diverticular status.
Diagnostic Pathways and Screening in the UK
The UK healthcare system uses the colonoscopy as a definitive diagnostic step following initial screening tests, such as the home-based Faecal Immunochemical Test (FIT). If a stool test detects microscopic amounts of blood, a colonoscopy is offered to find the source. Because both polyps and diverticula can occasionally cause minor bleeding, the colonoscopy provides the necessary clarity to determine the exact cause.
The GOV.UK health pages indicate that participation in national bowel screening programmes is vital for identifying polyps and other bowel conditions early, even in individuals who have no symptoms. By using a single procedure to investigate an abnormal screening result, the NHS can identify high-risk growths and common structural issues like diverticulosis simultaneously. This efficient use of diagnostic resources ensures that patients receive a full picture of their bowel health, allowing for coordinated follow-up care that may include regular polyp surveillance and dietary management for diverticular disease.
Long-term Management After Dual Detection
Following a colonoscopy where both polyps and diverticula were found, the patient is entered into a structured management plan that addresses the different needs of each condition. For the polyps, the laboratory results will dictate how soon the patient needs their next “surveillance” colonoscopy. For the diverticula, the focus shifts to preventing future episodes of diverticulitis through lifestyle and dietary adjustments.
UK clinical guidance typically focuses on:
- Fibre Intake: Gradually increasing dietary fibre to help waste move easily and reduce pressure on diverticula.
- Hydration: Drinking plenty of fluids to support the action of fibre and maintain soft stools.
- Vigilance: Monitoring for symptoms of a flare-up, such as localised abdominal pain or fever.
- Participation: Continuing with all invited bowel screening tests as scheduled by the healthcare provider.
By managing both conditions proactively, individuals can reduce the likelihood of complications from diverticular disease while ensuring that any new polyps are caught and removed in the future. This dual-focus approach ensures that the functional and cellular health of the large intestine is maintained throughout the patient’s later years.
Conclusion
A colonoscopy can detect both colon polyps and diverticulitis simultaneously, providing a comprehensive assessment of the bowel’s structural and cellular health. While polyps grow inward and are typically removed during the procedure, diverticula are outward-bulging pouches that are documented for long-term management. In the UK, this procedure is the gold standard for investigating bowel symptoms and abnormal screening results, although it is avoided during active inflammatory flare-ups for safety reasons. Identifying both conditions at once allows for a coordinated care plan focused on cancer prevention and the reduction of inflammatory risks. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a colonoscopy miss polyps if I have many diverticula?
In a colon with many pouches, it can be more challenging to see everything, but UK clinicians are trained to perform a thorough inspection and may use specialised techniques to ensure no growths are hidden.
Why can’t diverticula be removed during a colonoscopy like polyps?
Diverticular pouches involve the whole thickness of the bowel wall, so removing them would create a hole in the colon, whereas polyps are just extra tissue on the inner lining.
Is the preparation for a colonoscopy different if I have diverticulitis?
The bowel cleansing preparation is generally the same, but if you have a history of diverticulitis, your doctor will ensure you are fully recovered before the test.
Will a colonoscopy hurt more if I have diverticula?
The presence of diverticula can sometimes make the bowel more “loopy,” which may cause slight discomfort, but the clinical team uses sedation or pain relief to keep you comfortable.
If my colonoscopy shows only diverticula, do I still need screening?
Yes, you should still participate in all national screening programmes, as new polyps can develop over time even if your pouches remain stable.
Does having both conditions mean I need surgery?
Usually not; most polyps are removed during the colonoscopy, and diverticular disease is typically managed with diet unless severe complications occur.
Can a CT scan find polyps as well as a colonoscopy?
A CT colonography can find larger polyps, but it cannot find very small ones as effectively as a colonoscopy, and it cannot remove them.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the detection of polyps and diverticulitis via colonoscopy, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in internal medicine, general surgery, and emergency care. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.