

Yes, neuropathy is frequently misdiagnosed due to the fact that its primary symptoms, numbness, tingling, and weakness, are shared by several other medical conditions. In a clinical setting, these are known as mimics. In the United Kingdom, clinicians must carefully differentiate between systemic nerve damage and localized issues like poor circulation or spinal compression.
Because the peripheral nervous system is integrated with the vascular and musculoskeletal systems, a problem in one often feels like a problem in the other. This article explores the most common conditions mistaken for neuropathy and the diagnostic markers used to tell them apart.
What We Will Discuss In This Article
- Peripheral Artery Disease: Why poor blood flow mimics nerve pain
- Spinal Stenosis and Radiculopathy: Nerve compression versus nerve disease
- Fibromyalgia: Central versus peripheral pain processing
- Multiple Sclerosis: Central nervous system involvement
- The NHS Diagnostic Process: How clinicians rule out mimics
- Emergency guidance for sudden neurological or vascular crises
Peripheral Artery Disease (PAD)
- The Overlap: Both PAD and neuropathy cause pain, tingling, and heaviness in the legs and feet.
- The Difference: PAD pain, known as claudication, typically occurs during exercise and is relieved by rest. Neuropathic pain is often constant or worse at night. A clinician will check for a pulse in the feet; a weak pulse suggests a circulation issue rather than a primary nerve problem.
Spinal Stenosis and Radiculopathy
Issues in the spine can mimic peripheral neuropathy because the nerves that travel to your feet and hands all originate in the spinal cord.
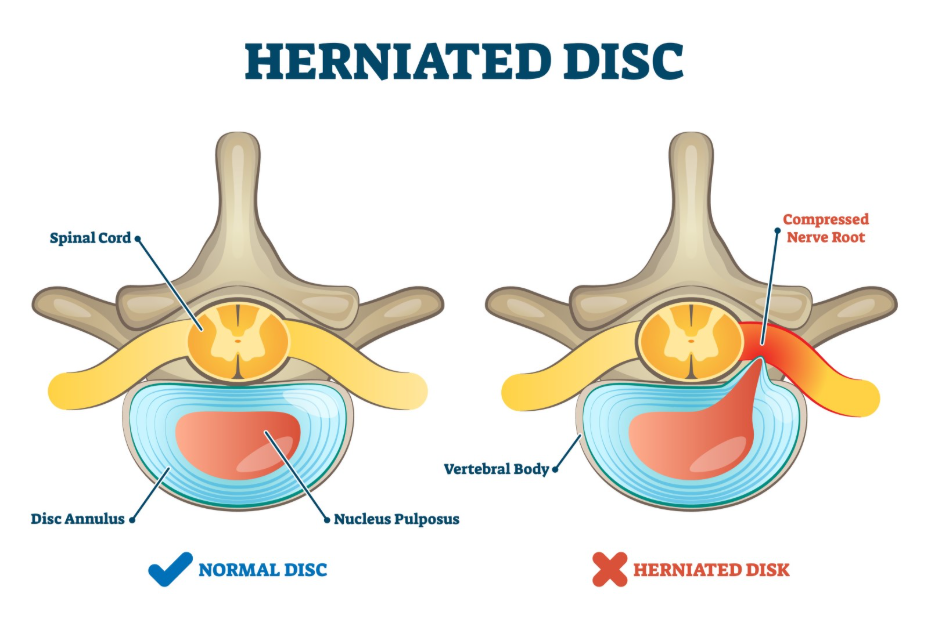
Radiculopathy
If a disc in your lower back is herniated, it can press on a nerve root. This causes pain and numbness to radiate down the leg, which can be mistaken for systemic neuropathy. This is commonly referred to as sciatica.
Spinal Stenosis
Narrowing of the spinal canal can put pressure on the nerves, causing leg weakness and tingling. Unlike peripheral neuropathy, which usually affects both feet equally, spinal issues often affect one side more than the other and may improve when you lean forward.
Fibromyalgia and Central Sensitisation
Fibromyalgia is a condition characterized by widespread musculoskeletal pain. Because it often involves tingling and a heightened sensitivity to touch, it is frequently confused with small fibre neuropathy.
- The Difference: In neuropathy, there is actual physical damage to the nerve fibres. In fibromyalgia, the nerves are physically intact, but the brain and spinal cord are processing pain signals incorrectly. A skin biopsy can distinguish between the two by checking for a reduced density of nerve endings, which is only present in true neuropathy.
Multiple Sclerosis (MS)
MS is an autoimmune condition where the immune system attacks the protective coating of the nerves in the brain and spinal cord.
- The Mimicry: MS often starts with numbness and tingling in the limbs, similar to peripheral neuropathy.
- The Clinical Marker: MS is a disease of the Central Nervous System, whereas peripheral neuropathy affects the nerves outside the brain and spine. Clinicians like Dr. Rebecca Fernandez look for other MS markers, such as vision changes or sudden coordination issues, which are not typical for simple peripheral neuropathy.
Diagnosis and Clinical Differentiation
To avoid misdiagnosis, UK physicians follow a structured protocol:
- Pulse Checks and ABI: Using an Ankle Brachial Index to rule out circulation problems.
- Imaging: MRI scans of the spine to look for nerve compression.
- Electrodiagnostic: Nerve Conduction Studies can confirm if the peripheral nerve itself is the source of the problem.
- Blood Panels: Screening for B12 deficiency or diabetes to confirm a metabolic cause for nerve damage.
Emergency Guidance
Certain mimics, such as a blood clot or acute spinal compression, are medical emergencies. Seek emergency care immediately if you experience:
- A leg or arm that suddenly becomes cold, pale, and pulseless
- Sudden and total loss of bladder or bowel control
- Numbness in the saddle area around the inner thighs and groin
- Severe weakness that prevents you from lifting your foot
- Signs of a silent heart attack such as sudden nausea and profound weakness
In these situations, call 999 or attend your nearest Accident and Emergency department immediately.
To Summarise
Neuropathy is frequently misdiagnosed because its symptoms overlap with circulation issues, spinal disorders, and central pain conditions. In the UK, a thorough clinical evaluation involving pulse checks, spinal imaging, and electrical nerve testing is essential to ensure the correct diagnosis. Distinguishing between these conditions is vital, as the treatment for a circulation problem is vastly different from the treatment for diabetic nerve damage. If you have persistent sensory changes, a comprehensive review of both your vascular and neurological health is the best path forward.
Can I have both neuropathy and poor circulation?
Yes. In fact, people with diabetes often suffer from both. This makes diagnosis and treatment more complex, as both conditions contribute to foot pain and the risk of ulcers.
Why did my MRI come back normal if I have numbness?
A normal spinal MRI rules out a slipped disc or stenosis as the cause. It does not rule out peripheral neuropathy, which occurs in the small branches of the nerves far away from the spine.
Is fibromyalgia a type of neuropathy?
No. Fibromyalgia is a disorder of pain processing in the brain. Neuropathy is a physical disease of the peripheral nerve fibres themselves.
Can anxiety cause symptoms that look like neuropathy?
Severe anxiety can cause hyperventilation, which leads to tingling in the hands and around the mouth. However, this is temporary and does not cause the persistent sensory loss or weakness seen in true neuropathy.
Authority Snapshot
This article was reviewed by Dr. Rebecca Fernandez, a UK trained physician with an MBBS and extensive experience in internal medicine, surgery, and emergency care. Dr. Fernandez has managed critically ill patients and stabilized acute trauma cases, providing her with a deep clinical understanding of the diagnostic overlap between vascular, spinal, and neurological emergencies. Her background in evidence based psychiatry ensures a holistic perspective on differentiating between physical nerve damage and central pain processing disorders.
