


In clinical practice across the United Kingdom, the term sinus headache is one of the most frequently misapplied diagnoses. While many people believe their facial pain and congestion are due to sinus inflammation, clinical data suggests that up to 90 percent of self-diagnosed sinus headaches are actually migraines. This confusion occurs because migraines can trigger the autonomic nervous system, leading to nasal discharge and pressure in the face. Distinguishing between these two is critical, as treating a migraine with decongestants will not provide long-term relief.
As a physician with experience in internal medicine, emergency care, and psychiatry, I often see patients who have spent months treating a suspected infection when the root cause is neurological. Understanding the anatomical and symptomatic differences between these conditions is essential for an accurate diagnosis. This article clarifies the clinical markers of true sinusitis versus migraine.
What We Will Discuss In This Article
- Defining True Sinusitis: Inflammation and infection
- The Migraine Mimic: Why migraines cause facial pressure
- Key Clinical Differences: Fever and discharge vs. nausea and light sensitivity
- Anatomical Overlap: The trigeminal nerve and facial pain
- Diagnostic Red Flags: When facial pain requires urgent care
- Integrated Management: Choosing the right treatment pathway
Defining True Sinus Headache
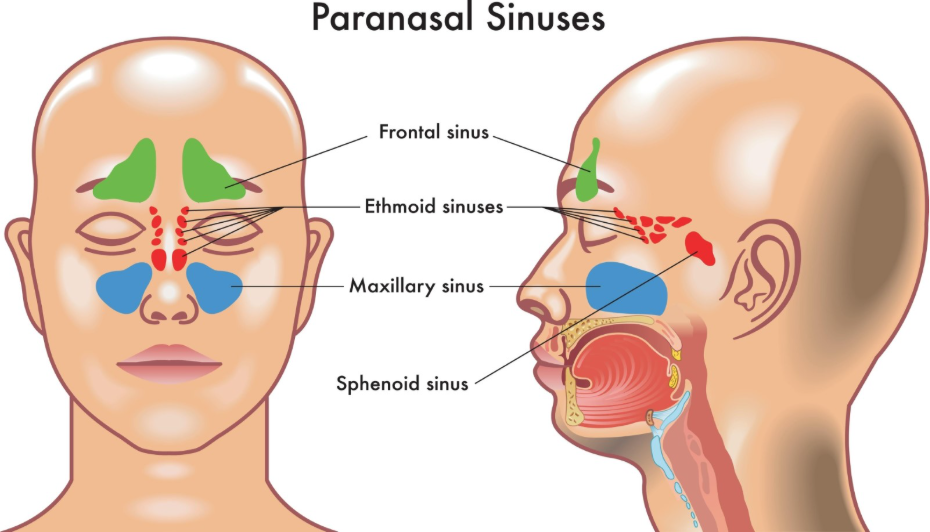
A true sinus headache, formally known as rhinosinusitis, is a secondary headache caused by an infection or inflammation of the paranasal sinuses. For a diagnosis of sinus headache to be clinically accurate, there must be evidence of an active sinus issue.
Symptoms of a true sinus headache usually include a thick, discoloured (yellow or green) nasal discharge, a reduced sense of smell, and pain that is localized over the affected sinus. Most importantly, these headaches are almost always accompanied by systemic signs of infection, such as a fever. Once the underlying infection is treated with antibiotics or decongestants, the headache should resolve within seven days.
The Migraine Mimic
The reason migraines are so often mistaken for sinus issues is due to the activation of the trigeminal nerve. This nerve supplies sensation to the face, including the areas over the sinuses. When a migraine attack begins, it can cause:
- Facial Pressure: Often felt behind the eyes or in the cheeks.
- Nasal Congestion: A clear, watery nasal discharge.
- Eye Watering: Redness or tearing of the eyes.
Key Clinical Differences
To untangle these conditions, we look for specific diagnostic markers:
- Nasal Discharge: In a sinus infection, discharge is thick and discoloured. In a migraine, it is clear and watery.
- Systemic Symptoms: Fever and chills point to a sinus infection. Nausea and light sensitivity point to a migraine.
- Duration: Sinus headaches usually last for days or weeks until the infection clears. Migraines typically last 4 to 72 hours.
- Triggers: Migraines are often triggered by stress, weather changes, or certain foods, whereas sinus headaches follow a cold or an allergy flare up.
The Role of Psychological Well-being
Given my background in psychiatry and mindfulness-based therapies, I frequently observe that chronic facial pain—regardless of the cause—can lead to significant anxiety and health-seeking behaviour. Integrating stress management and mindfulness can be particularly helpful for migraine patients who experience frequent facial pressure, as it helps calm the autonomic nervous system responses that lead to nasal symptoms.
Emergency Guidance: Identifying Red Flags
While most facial pain is not life threatening, some symptoms require immediate intervention. Seek emergency care immediately if you experience:
- Periorbital Swelling: Redness or swelling around the eye or eyelids.
- Vision Changes: Sudden double vision or loss of vision.
- Neurological Signs: Confusion, severe drowsiness, or a stiff neck.
- High Fever: A temperature that does not respond to standard medication.
- Signs of a Silent Heart Attack: Such as sudden nausea and profound weakness.
In these situations, call 999 or attend your nearest Accident and Emergency department immediately.
To Summarise
The primary difference between a sinus headache and a migraine is the presence of an infection. A true sinus headache involves fever and discoloured discharge, while a migraine involves sensory sensitivities and clear nasal symptoms. In the UK, clinicians like Dr. Rebecca Fernandez emphasize that misdiagnosing a migraine as a sinus problem leads to ineffective treatment and prolonged suffering. By identifying the clear clinical markers of each condition, you can ensure you are treating the correct underlying cause and protecting your long-term health.
Can allergies cause a migraine?
Yes. While allergies cause sinus inflammation, the systemic stress of an allergic reaction can act as a powerful trigger for a migraine attack.
Why does my face hurt when I have a migraine?
The trigeminal nerve, which is the main pathway for migraine pain, has branches that cover your forehead, cheeks, and jaw. When this nerve is irritated, you feel pain in these facial regions.
Will a decongestant help a migraine?
It might temporarily relieve the nasal congestion, but it will not stop the underlying neurological process of the migraine. This is why many people find that sinus medications only provide partial relief.
How do I know if I need antibiotics?
If you have a fever, thick green discharge, and facial pain that has lasted more than ten days, you should consult your GP to see if an antibiotic is required for a bacterial sinus infection.
Authority Snapshot
This article was reviewed by Dr. Rebecca Fernandez, a UK-trained physician with an MBBS and a diverse background in internal medicine, emergency care, and psychiatry. Dr. Fernandez has extensive experience in managing acute trauma and stabilising critically ill patients. Her expertise in patient assessment and her dedication to integrating digital health solutions and mindfulness-based therapies ensure that this guide to sinus pain and migraine is clinically precise and focused on holistic care.


