


A brain tumour can be treated without traditional surgery in specific clinical circumstances, such as when the growth is slow-growing, located in a high-risk area, or responsive to non-invasive therapies like radiotherapy. In the United Kingdom, healthcare professionals utilise a multidisciplinary approach to determine whether a surgical or non-surgical pathway is the most appropriate for a patient’s specific diagnosis. While surgical removal is a common primary intervention, many patients successfully manage their condition through active surveillance, medication, or targeted radiation techniques. The UK healthcare system follow evidence-based protocols established by the NHS and NICE to ensure that all management decisions prioritise the preservation of neurological function and the patient’s overall quality of life. This article explores the various non-surgical management options available within the NHS and explains how clinical teams coordinate care when an operation is not the preferred route. Understanding these alternatives provides a comprehensive view of the integrated care pathways used to manage complex neurological conditions in the UK.
What We’ll Discuss in This Article
- The role of active surveillance (watch and wait) for stable tumours.
- Using radiotherapy as a primary non-surgical management tool.
- The application of stereotactic radiosurgery for deep-seated masses.
- Medical management and hormone therapy for specific tumour types.
- Chemotherapy and systemic treatments for certain malignant growths.
- How UK clinical teams assess the risks and benefits of non-surgical care.
Active Surveillance: The Watch and Wait Approach
Active surveillance is a non-surgical management strategy used in the United Kingdom for brain tumours that are slow-growing, benign, or not currently causing symptoms. This approach involves monitoring the tumour with regular imaging rather than proceeding to immediate surgery or radiation. The NHS states that if a brain tumour is slow-growing and not causing symptoms, it may be monitored with regular scans rather than being treated immediately.
During this period, patients remain under the care of a specialist team and undergo scheduled MRI scans to detect any changes in the size or characteristics of the mass. This pathway is frequently used for small meningiomas or acoustic neuromas where the risks of an operation may outweigh the benefits of removal. If the scans show that the tumour is stable and the patient remains asymptomatic, active surveillance can continue for many years. However, if growth is detected or the patient develops new neurological signs, the multidisciplinary team will re-evaluate the plan and may recommend transitioning to active treatment. This integrated surveillance ensures that clinical intervention is only performed when it is medically necessary.
Radiotherapy as a Primary Treatment Modality
Radiotherapy is a highly effective non-surgical treatment used in the UK to manage various brain tumours by using high-energy radiation beams to destroy abnormal cells. It can be used as the main management for tumours that are difficult to reach surgically or for patients who are not physically fit for a major operation. NICE clinical guidelines for brain tumours indicate that radiotherapy should be considered for patients with tumours where surgery is not possible or carries an unacceptably high risk of neurological deficit.
| Treatment Type | Method | Primary Use in UK |
| External Beam | Daily sessions over weeks. | Inoperable gliomas; diffuse growths. |
| Stereotactic (SRS) | Single high-dose session. | Small, well-defined tumours. |
| Proton Beam | Precise particle therapy. | Specific paediatric or skull-base cases. |
Modern radiotherapy techniques allow for extreme precision, ensuring the maximum dose reaches the tumour while minimising the impact on the surrounding healthy brain. For some patients, this treatment can successfully stop the growth of the mass or even cause it to shrink over time. In the UK, specialists use detailed computerised planning and bespoke masks to ensure that the radiation is delivered with millimetre accuracy. This non-invasive option provides a vital alternative for managing tumours that were previously considered untreatable.
Stereotactic Radiosurgery (SRS)
Stereotactic radiosurgery is a specialised form of radiation treatment that can manage small brain tumours without the need for a surgical incision or a general anaesthetic. Despite its name, radiosurgery is not a traditional operation; instead, it uses multiple tiny beams of radiation that converge on a single point to deliver a high dose to the tumour. This causes the abnormal cells to stop dividing, effectively “neutralising” the growth.
In the United Kingdom, SRS is a common non-surgical option for small, deep-seated tumours such as acoustic neuromas or limited brain metastases. Because the procedure is highly targeted, it spares the healthy brain tissue nearby, which is essential when a tumour is located near critical structures like the brainstem. Most patients in the UK can have this treatment as a day case, allowing them to return home shortly after the procedure. Over several months, the treated tumour typically becomes inactive scar tissue. This advanced technology has significantly expanded the non-surgical options available within the NHS for complex neurological cases.
Medical Therapy for Hormone-Producing Tumours
Certain types of brain tumours, particularly those affecting the pituitary gland, can often be managed entirely through medication without the need for any surgery or radiation. These tumours, known as functioning adenomas, can cause health issues by overproducing hormones, and specific drugs can be used to block this production and shrink the mass. The GOV.UK health pages provide clinical profiles indicating that for certain pituitary tumours, medical therapy can normalise hormone levels and reduce tumour size effectively.
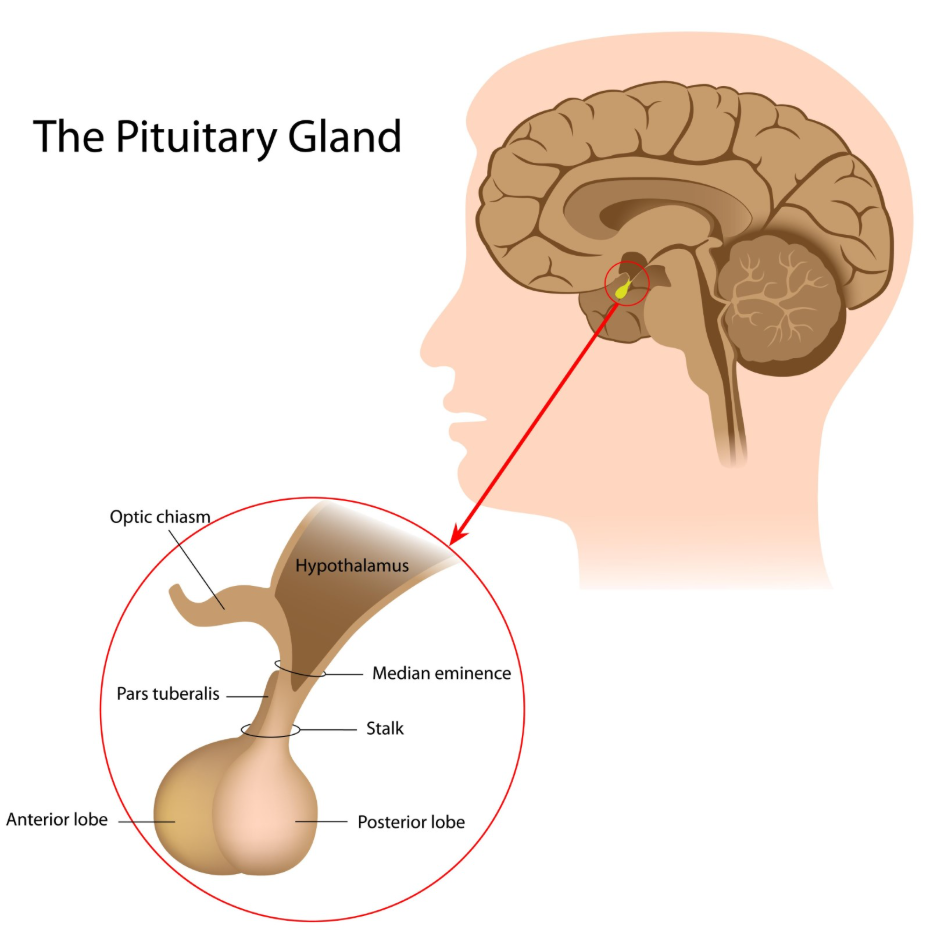
For example, prolactinomas are frequently treated with dopamine agonist medications that are taken as tablets. These drugs work by mimicking the natural chemicals that regulate the master gland, often causing the tumour to shrink significantly. In the UK, endocrinologists lead the management of these cases, using regular blood tests to monitor hormone levels. Surgery is generally only considered if the medication is not tolerated or if the tumour is pressing on the optic nerves and threatening vision. This pharmaceutical-led approach highlights how understanding the biological nature of a tumour can lead to successful non-surgical outcomes.
Chemotherapy and Systemic Management
Chemotherapy and targeted systemic therapies are used in the United Kingdom to manage specific brain tumours that are sensitive to chemical agents, often providing a non-surgical route for certain malignant conditions. Some primary brain tumours, such as primary central nervous system lymphoma or specific germ cell tumours, are highly responsive to chemotherapy and may be treated primarily with medication rather than surgery.
For other types of high-grade tumours, chemotherapy is used alongside radiotherapy to enhance the overall effectiveness of the non-surgical management. The drugs work by travelling through the bloodstream to reach the tumour cells, interfering with their ability to divide. In the UK, medical oncologists manage these treatments in cycles, using regular blood tests to ensure the patient’s immune system remains healthy. While most brain tumours still require a biopsy for a definitive diagnosis, the subsequent management can often be entirely non-surgical if the tumour shows a good response to systemic therapy.
Integrated Decision Making and Risk Assessment
In the United Kingdom, the decision to treat a brain tumour without surgery is made through an integrated review by a Multidisciplinary Team (MDT). This team evaluates the imaging results, the patient’s symptoms, and their general fitness to decide whether an operation, radiation, or surveillance is the safest and most effective option.
The UK risk assessment process involves:
- Location Analysis: Determining if surgery would cause more harm than the tumour itself.
- Tumour Behaviour: Assessing whether the mass is slow-growing or aggressive.
- Patient Fitness: Evaluating the risks of general anaesthesia for the individual.
- Functional Preservation: Prioritising the maintenance of speech, motor skills, and vision.
This collaborative approach ensures that the management plan is tailored to the specific needs of the patient. If surgery is not the preferred route, the MDT will establish a clear non-surgical pathway with scheduled follow-ups and specialist support. By following these national standards, the NHS provide a robust safety net for patients, ensuring they receive the most appropriate care based on the latest clinical evidence.
Conclusion
A brain tumour can be treated without surgery through methods such as active surveillance, radiotherapy, or medical therapy, depending on its specific biological characteristics. In the UK, the NHS prioritises non-surgical routes for stable, asymptomatic tumours and for those located in high-risk areas where an operation may cause neurological damage. Advanced technologies like stereotactic radiosurgery and hormone-blocking medications provide precise and effective alternatives to traditional neurosurgery. Every management plan is designed by a multidisciplinary team to ensure the best possible balance between tumour control and the preservation of health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a brain tumour go away on its own without surgery?
Primary brain tumours do not usually disappear without intervention, but they can remain stable and inactive for many years under active surveillance.
What is “watch and wait”?
This is a strategy of active surveillance where a stable tumour is monitored with regular MRI scans rather than being treated with surgery.
Is radiosurgery the same as a normal operation?
No; stereotactic radiosurgery uses precise radiation beams and does not involve an incision or a stay in hospital.
Are all pituitary tumours treated with surgery?
No; many pituitary tumours are managed very successfully with medication that regulates hormones and shrinks the mass.
Will radiotherapy make the tumour shrink?
Radiotherapy can cause some tumours to shrink, but its primary goal is often to stop the abnormal cells from dividing and growing further.
Can chemotherapy be used instead of surgery?
For most tumours, chemotherapy is used alongside other treatments, but for some specific types like lymphoma, it can be the primary management.
How do doctors decide if surgery is too risky?
Specialists assess if the tumour is in an “eloquent” area responsible for vital functions like speech or movement, where surgery could cause permanent damage.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding non-surgical treatments for brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience in surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


