


Abdominal bloating is a common experience that usually results from dietary factors or minor digestive issues. However, when the sensation of pressure or swelling becomes persistent and is accompanied by other specific changes in bodily function, it can indicate the need for a clinical investigation to rule out more serious underlying conditions, including certain types of cancer. Understanding the difference between temporary discomfort and symptoms that require medical evaluation is essential for maintaining long-term health.
What We’ll Discuss in This Article
- Differentiating between temporary and persistent bloating
- Red flag symptoms that require medical assessment
- The link between persistent bloating and ovarian health
- Bowel-related symptoms and their clinical significance
- Standard UK diagnostic pathways and screening tests
- The role of age and family history in risk assessment
Distinguishing Between Common and Persistent Bloating
Bloating that is considered a medical concern is typically characterised by being new, persistent, and occurring frequently over a short period. Most bloating related to diet or Irritable Bowel Syndrome fluctuates throughout the day, often worsening after meals and improving after passing wind or a bowel movement. In contrast, bloating that may be linked to a more serious condition tends to be present most of the time and does not easily resolve with standard lifestyle changes. Bloating that occurs for the first time or happens more than 12 times a month should be discussed with a healthcare professional to ensure there is no underlying cause.
In clinical practice, the duration of the symptom is a vital factor. If the abdomen feels swollen or tight for several weeks without significant intervals of relief, it is categorised as persistent. This is particularly relevant if the bloating occurs alongside physical distension, where the abdomen is visibly larger than normal. While gas and air are the most frequent causes of a “full” feeling, a medical review helps determine if the sensation is caused by something else, such as fluid accumulation or an internal mass.
Red Flag Symptoms and Clinical Indicators
A clinical review is essential if bloating is accompanied by “red flag” symptoms such as unintentional weight loss, persistent loss of appetite, or a change in bowel habits. These indicators suggest that the bloating is not a simple functional digestive issue but rather a sign of an organic process occurring within the body. Clinicians use these signs to prioritise patients for diagnostic imaging or specialist referrals to ensure that any potential malignancy is identified early.
Other warning signs include feeling full very quickly after starting a meal (early satiety) or experiencing persistent pain in the abdomen or pelvic area. Fever, night sweats, or a general feeling of being unwell can also accompany serious underlying issues. These symptoms are not typical for standard bloating and often indicate that the body is responding to an inflammatory or malignant process. When these factors are present together, a systematic investigation of the abdominal organs is usually the next clinical step.
Persistent Bloating and Ovarian Cancer Risks
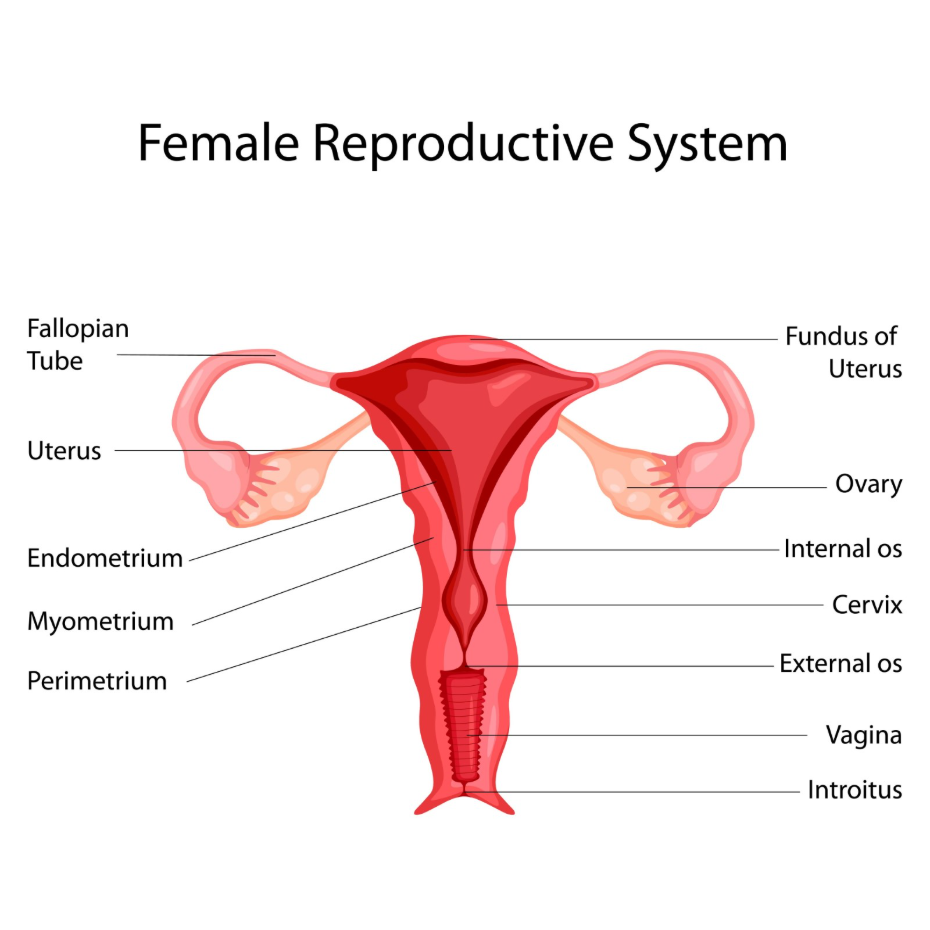
Persistent abdominal distension is one of the primary symptoms used to screen for ovarian health in women, particularly those over the age of 50 or those who have gone through menopause. In the United Kingdom, medical guidelines specify that a new onset of frequent bloating should be investigated through a blood test and an ultrasound scan. This is especially true if the bloating is accompanied by a persistent feeling of fullness, pelvic pain, or an increased frequency of urination. The National Institute for Health and Care Excellence provides clear pathways for the recognition and referral of suspected ovarian cancer based on persistent abdominal symptoms.
It is a common misconception that bloating related to ovarian issues will always be accompanied by severe pain. In many cases, the bloating is the first and most prominent symptom. Because these symptoms can mimic digestive disorders like Irritable Bowel Syndrome, it is important for women who have not previously been diagnosed with a bowel condition to seek an evaluation if these symptoms appear for the first time later in life. Diagnostic pathways are designed to rule out ovarian issues as a priority in these instances.
Bowel Habit Changes and Digestive Health
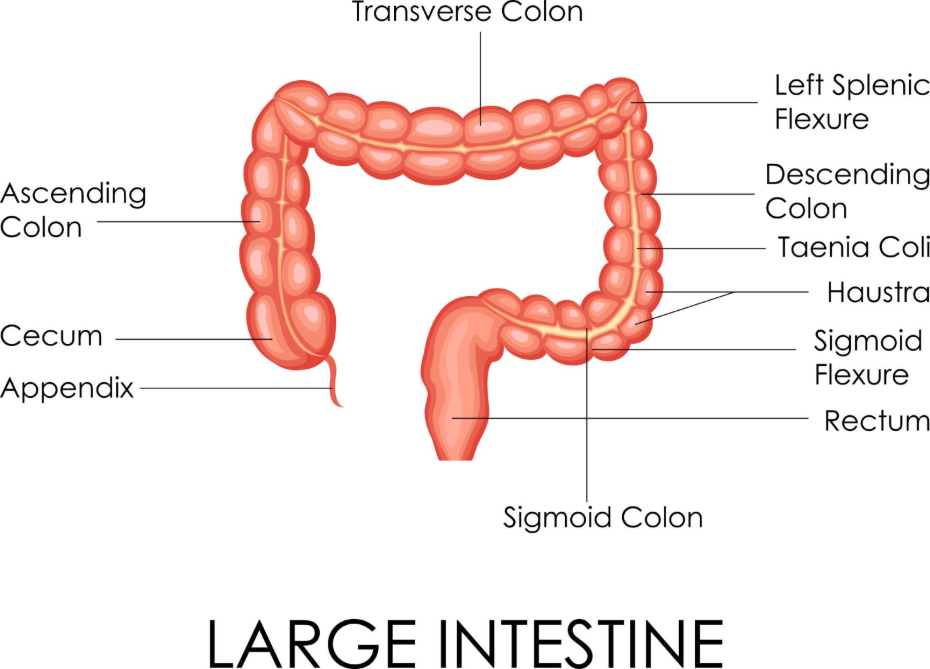
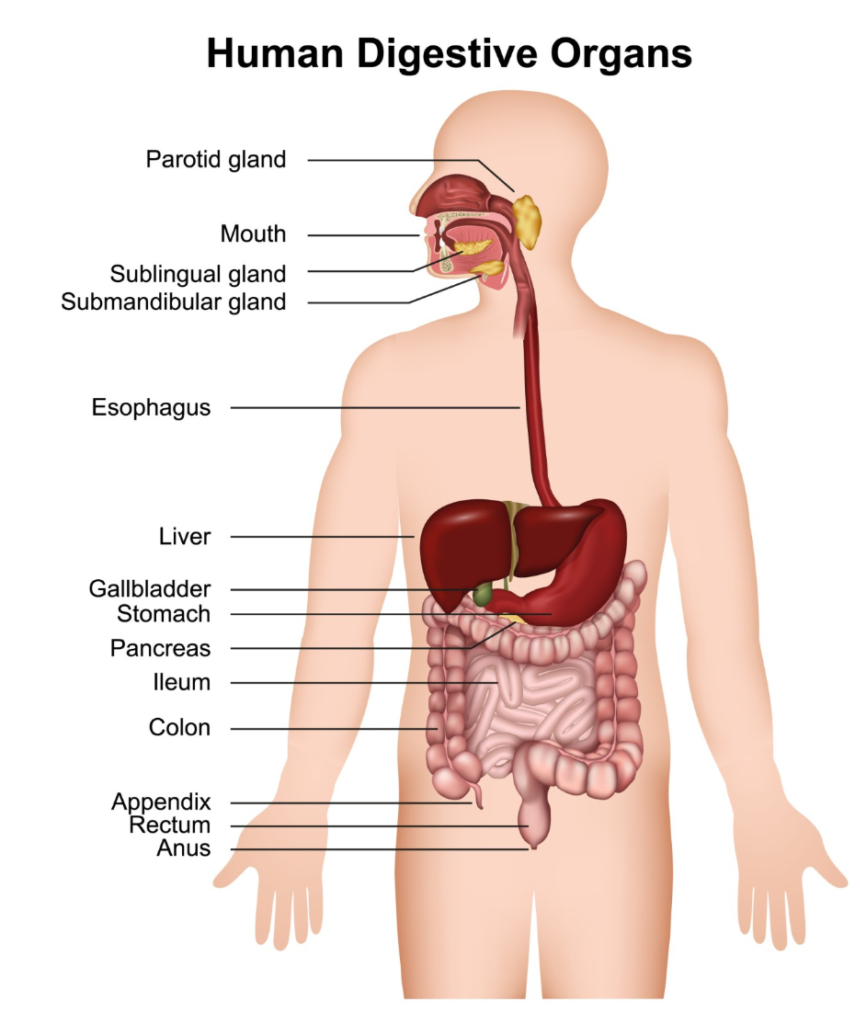
If bloating is combined with a lasting change in bowel habits, such as stools becoming more frequent, looser, or the presence of blood, it may indicate a need to investigate the health of the large intestine. While Irritable Bowel Syndrome can cause varied bowel patterns, a consistent shift toward abnormal stools that lasts for more than three weeks is a recognised clinical marker for further testing. This is particularly relevant for rule-out procedures concerning bowel cancer, where early detection is vital. Bowel cancer symptoms can include a persistent change in bowel habit, blood in the stool, or abdominal pain and bloating.
Diagnostic tools for these symptoms often include a Faecal Immunochemical Test (FIT), which checks for hidden blood in a stool sample. If the results are abnormal or if the clinical suspicion remains high, a colonoscopy may be performed to directly visualise the lining of the bowel. This procedure allows doctors to identify polyps or other abnormalities that could be causing the bloating and changes in bowel frequency. Monitoring the consistency of the stool using tools like the Bristol Stool Form Scale can also provide useful data for a medical assessment.
The Importance of Age and Medical History
The level of clinical concern regarding bloating often increases with age or if there is a significant family history of certain cancers. While bloating can affect individuals of any age, new and persistent symptoms in those over 50 are evaluated with greater scrutiny due to the higher statistical prevalence of underlying organic disease in this demographic. Medical history is a key component of the risk assessment conducted by healthcare professionals during an initial consultation.
A family history of ovarian, bowel, or breast cancer may prompt a healthcare provider to initiate investigations sooner to ensure all risks are adequately assessed. Genetic factors can sometimes increase the susceptibility to certain types of cancer, making it important to disclose any relevant family patterns. However, most cases of bloating in all age groups are eventually found to be related to non-cancerous causes, and the primary goal of testing is to provide an accurate explanation for the symptoms.
Standard Diagnostic Tests and Procedures
Healthcare professionals utilise a range of tests to determine the cause of persistent bloating, beginning with non-invasive screenings. A CA125 blood test is often the first step for women to check for a specific protein marker that can be elevated in various conditions, including ovarian cancer. It is important to note that CA125 can also be raised by non-cancerous conditions such as endometriosis or fibroids, so it is used as a screening tool rather than a final diagnosis.
If blood or stool tests indicate a need for further investigation, imaging is used to look at the abdominal and pelvic organs. An ultrasound scan is commonly used to examine the ovaries and uterus, while a CT scan may be used to provide a more detailed view of the entire abdomen. For bowel-related concerns, a colonoscopy or a flexible sigmoidoscopy allows for a direct examination of the intestinal lining. These procedures are part of a structured diagnostic pathway designed to identify the source of persistent bloating and ensure appropriate management.
Conclusion
Bloating is usually benign, but its persistence and frequency are key factors in determining when a clinical review is necessary. If the sensation of pressure is new, occurs frequently, and is paired with weight loss, loss of appetite, or changes in bathroom habits, it warrants a professional medical assessment. Following established UK diagnostic pathways helps ensure that serious conditions are identified or excluded as early as possible. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
What is meant by “persistent” bloating?
In a medical context, bloating is considered persistent if it is present most of the time for three weeks or more and does not fluctuate with dietary changes.
Can bloating be the only symptom of a serious illness?
While it can be the first symptom, serious conditions usually present with other signs over time, such as early satiety, weight loss, or abdominal pain.
How many times a month is bloating considered frequent?
UK clinical guidelines suggest that bloating occurring more than 12 times a month is a threshold for seeking a medical review, especially if it is a new symptom.
Does a high CA125 result always mean cancer?
No, CA125 is a marker of inflammation or irritation and can be elevated by many benign conditions such as pelvic inflammatory disease or even menstruation.
What is a “FIT” test?
A FIT (Faecal Immunochemical Test) is a stool test used to detect very small amounts of blood that may not be visible to the naked eye, often used to screen for bowel health.
Is bloating a common symptom of menopause?
Yes, hormonal changes during menopause can cause bloating, but it is important not to assume it is hormonal if the bloating is new and persistent.
Can stress cause the same type of bloating as serious conditions?
Stress can cause significant bloating through the gut-brain axis, but it is typically not associated with “red flag” symptoms like unexplained weight loss or blood in the stool.
Authority Snapshot (E-E-A-T)
This medical education content is designed to provide accurate, evidence-based information for the UK public regarding the symptoms of bloating. The material is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience across internal medicine, general surgery, and acute care. All information provided is strictly aligned with the clinical standards and diagnostic pathways set by the NHS and the National Institute for Health and Care Excellence (NICE).


