


Abdominal bloating is an extremely common experience that most people encounter at some point, often resulting from dietary habits or temporary digestive disruptions. However, when bloating becomes persistent, recurrent, or painful, it can lead to concerns about whether the cause is a functional issue like irritable bowel syndrome or a more significant underlying health condition. Distinguishing between these possibilities involves a careful evaluation of the nature of the bloating, the presence of accompanying symptoms, and an understanding of established clinical markers used in the United Kingdom health system.
What We’ll Discuss in This Article
- Typical features of bloating associated with Irritable Bowel Syndrome
- Red flag symptoms that differentiate functional issues from organic disease
- Specific considerations for persistent bloating and ovarian health in women
- Common medical conditions with symptoms that overlap with functional gut issues
- Clinical pathways used by healthcare professionals for diagnostic investigation
- Standard laboratory tests used to rule out inflammation or malabsorption
Characteristics of Bloating in Irritable Bowel Syndrome
Bloating in Irritable Bowel Syndrome is usually a functional symptom related to how the digestive system moves gas and waste rather than a sign of structural damage. In this context, the term functional means that while the digestive tract appears normal under physical examination or imaging, the way it operates is altered. For individuals with this condition, bloating is often described as a sensation of internal pressure that fluctuates throughout the day, frequently worsening after meals and improving following a bowel movement or the passage of wind.
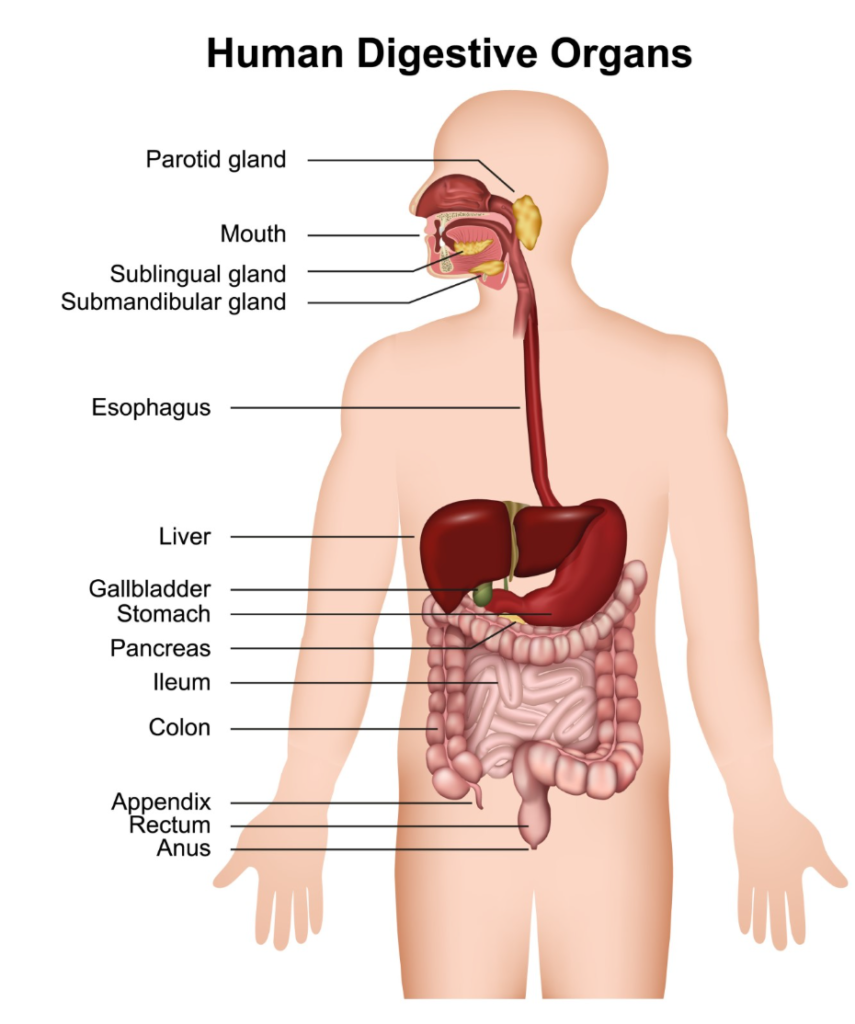
The physiological mechanism behind this type of bloating often involves visceral hypersensitivity, where the nerves in the gut are overly sensitive to normal amounts of gas or the stretching of the intestinal walls. It is also frequently linked to the fermentation of certain carbohydrates by gut bacteria, which releases gas as a byproduct. Because this condition does not cause physical inflammation or permanent damage to the gut lining, the bloating is typically not associated with systemic symptoms like fever or significant, unintended weight loss.
Differentiating Functional Bloating from Organic Disease
Identifying red flag symptoms is the primary method used by clinicians to determine if abdominal swelling requires investigation for more serious conditions. While functional bloating is uncomfortable, it does not typically interfere with sleep or cause a decline in overall physical health. In contrast, organic diseases, such as inflammatory conditions or malignancies, often present with systemic indicators that suggest a more aggressive process is occurring within the body.
Medical professionals pay close attention to symptoms that occur at night, such as being woken up by abdominal pain or the need to pass a stool. Other significant indicators include blood in the stool, a persistent change in bowel habits lasting more than a few weeks, or unexplained anaemia identified through blood tests. Bloating is most often caused by a buildup of gas in the digestive system, which can be linked to specific foods or habits like swallowing too much air. When bloating is accompanied by these additional factors, it moves out of the category of a simple functional issue and requires a more detailed clinical assessment.
Persistent Bloating and Ovarian Health
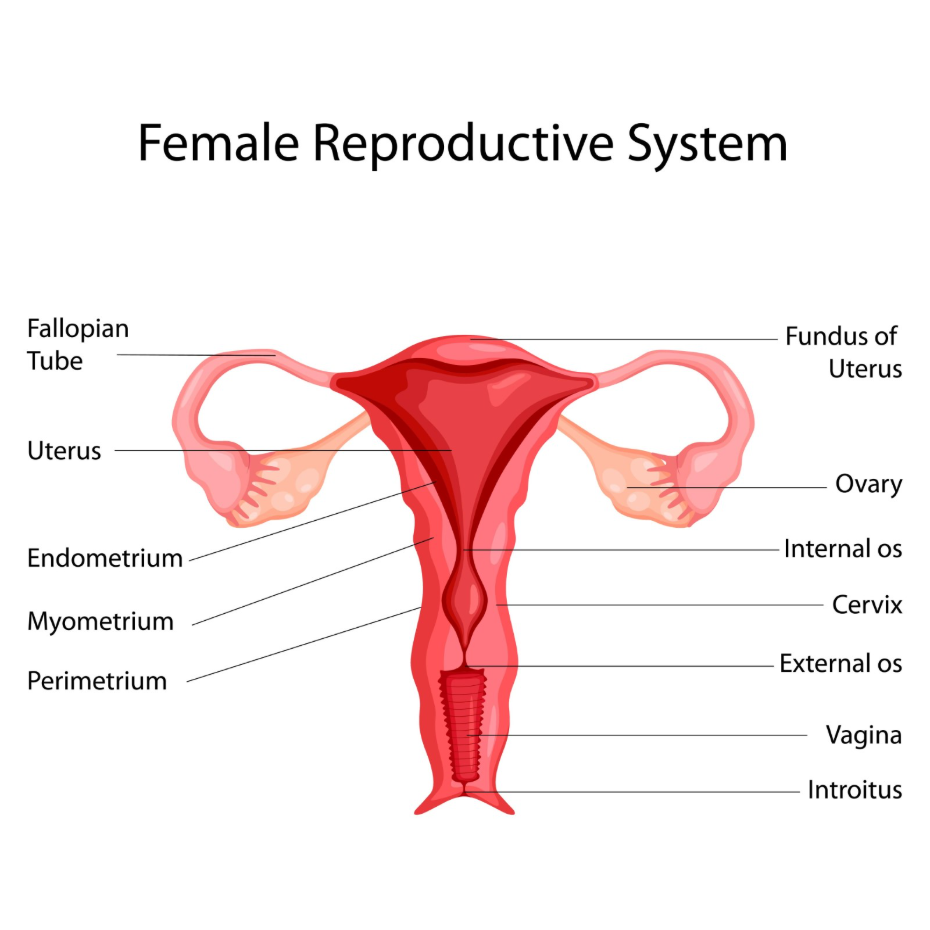
Persistent or frequent bloating in women is treated with specific clinical suspicion to exclude potential ovarian health issues, particularly if the symptom is new. National guidelines in the UK emphasise that bloating which occurs more than twelve times per month, especially in women over the age of fifty, should not be dismissed as a simple digestive issue. This is because bloating can be an early indicator of ovarian cancer, a condition where early detection significantly influences long-term outcomes.
Shutterstock
Explore
Healthcare professionals follow a specific pathway for women presenting with new and persistent abdominal distension. The National Institute for Health and Care Excellence provides guidelines on the recognition and referral for suspected cancer, including the use of CA125 blood tests and ultrasound scans for women with persistent bloating. This clinical vigilance ensures that symptoms are not mistakenly attributed to menopause or Irritable Bowel Syndrome without first ruling out more serious gynaecological concerns.
Inflammatory and Autoimmune Causes of Abdominal Distension
Conditions that cause malabsorption or inflammation, such as coeliac disease and Crohn’s disease, can present with bloating that is distinct from functional digestive issues. Coeliac disease is an autoimmune condition where the body reacts to gluten, causing damage to the small intestine. This damage prevents the proper absorption of nutrients, leading to a buildup of undigested material and gas, which manifests as persistent bloating, foul-smelling stools, and nutritional deficiencies.
Inflammatory Bowel Disease, which includes Crohn’s disease and ulcerative colitis, involves physical inflammation and ulceration of the digestive tract. The bloating in these cases is often accompanied by severe abdominal pain, fatigue, and sometimes a palpable mass in the abdomen. The National Institute for Health and Care Excellence recommends specific testing, such as faecal calprotectin, to distinguish between irritable bowel syndrome and inflammatory bowel disease. These tests measure a protein found in the stool that serves as a marker for active inflammation in the bowel.
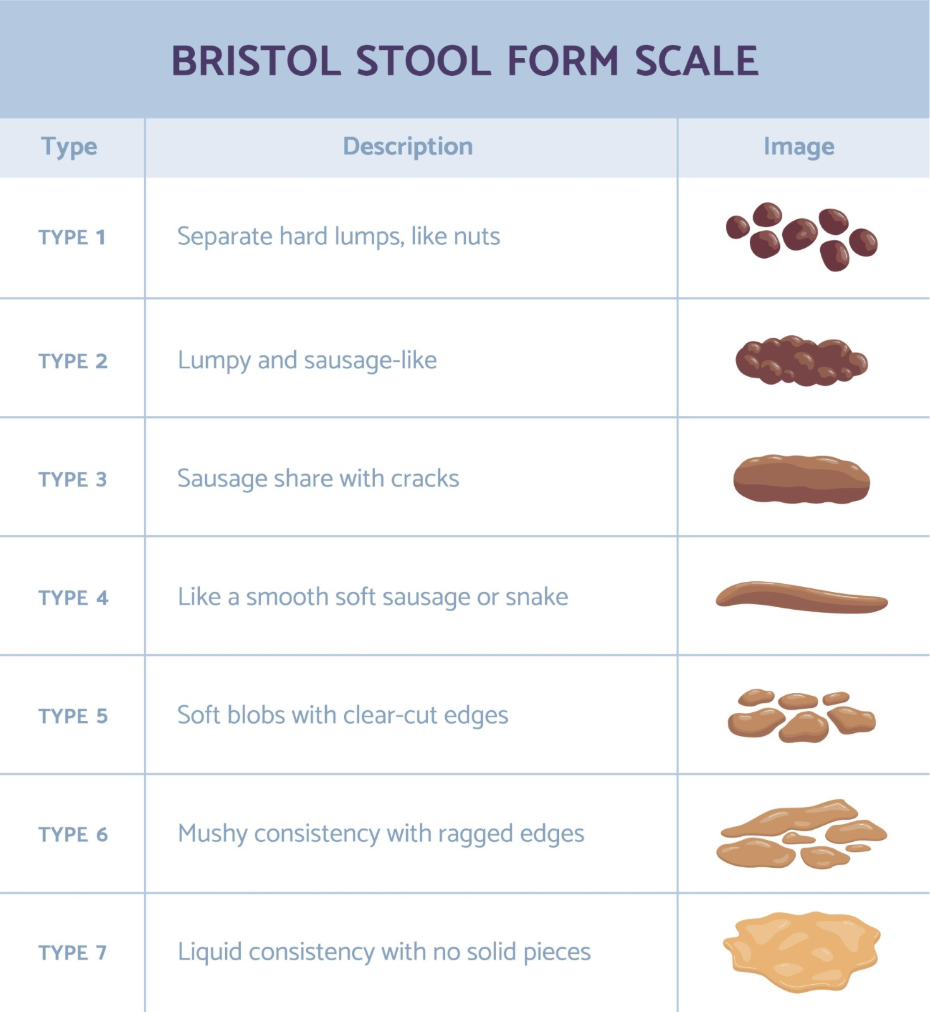
Understanding the Bristol Stool Form Scale and Bowel Habit
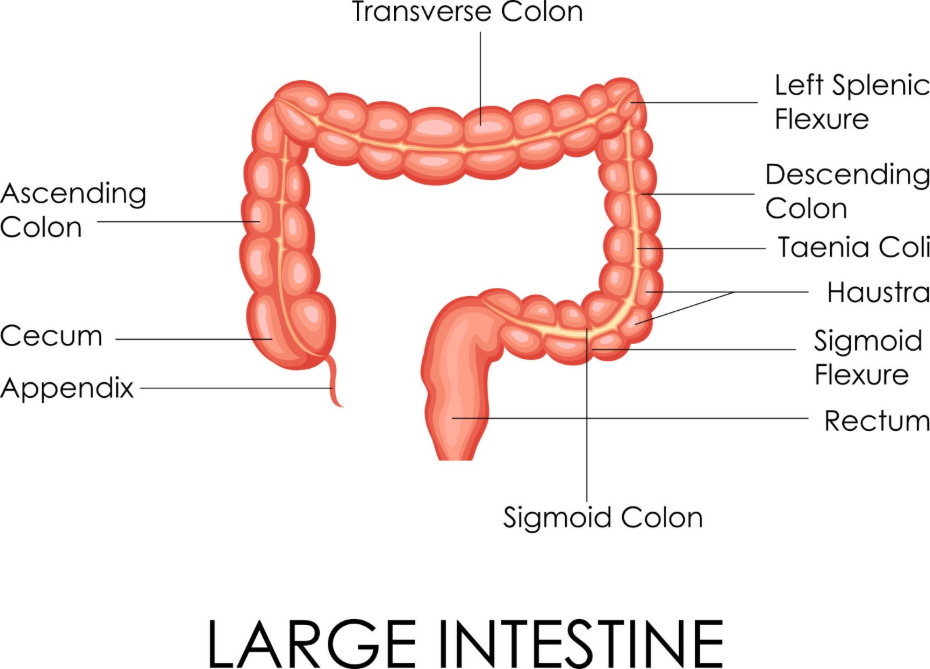
The consistency and frequency of bowel movements provide essential clues as to whether bloating is part of a functional syndrome or a symptom of a structural issue. In functional disorders, bloating is often tied to constipation or diarrhoea, but the stool consistency usually falls within the range of the Bristol Stool Form Scale without containing blood or excessive mucus. Persistent constipation can lead to a backlog of stool, which traps gas and causes the abdomen to feel stretched and tight.
If the bloating is accompanied by a permanent change in stool consistency, such as stools becoming consistently thinner or more frequent over a period of three weeks, it requires a different level of medical attention. Clinicians use these patterns to determine if an individual needs a referral for a colonoscopy or other imaging. While IBS can cause varied stool patterns, a change that only moves in one direction (becoming progressively more abnormal) is generally considered more suspicious than the fluctuating patterns typical of functional gut issues.
Clinical Investigation Pathways and Standard Tests
Medical professionals use a structured series of tests to evaluate whether bloating is a functional symptom or a sign of an underlying clinical condition. The diagnostic process usually begins in primary care with a thorough history and a physical examination of the abdomen to check for tenderness or swelling. If the bloating is persistent, a clinician will typically order a suite of blood tests to look for signs of a wider issue.
Standard investigations often include a Full Blood Count to check for anaemia and a C-reactive protein test to screen for systemic inflammation. Specific antibody tests for coeliac disease are also a routine part of the investigation for persistent bloating. If these initial screens are normal and there are no red flag symptoms, a diagnosis of a functional disorder may be considered. However, if any markers are abnormal, the clinical pathway will lead to more specialised tests, such as imaging or endoscopy, to directly visualise the internal structures of the digestive or reproductive systems.
Conclusion
Differentiating between bloating caused by Irritable Bowel Syndrome and more serious conditions relies on identifying the duration, frequency, and accompanying symptoms. While most bloating is related to functional gut issues and diet, new and persistent symptoms require a methodical clinical approach to ensure inflammatory or malignant conditions are excluded. Understanding the established medical markers and red flags allows for a more focused assessment of digestive health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is it normal for IBS bloating to be worse in the evening?
It is common for functional bloating to increase throughout the day as gas accumulates from meals, often being most prominent by the evening.
What is the difference between bloating and distension?
Bloating is the internal sensation of pressure, whereas distension is the visible increase in abdominal size that can be measured or seen.
Can stress make bloating worse in both IBS and serious conditions?
Stress affects the gut-brain axis and can worsen the sensation of bloating in any condition, though it is a primary driver in functional disorders like IBS.
How long should I wait before seeking advice for new bloating?
In the UK, persistent bloating that occurs frequently for more than three weeks is usually the threshold for a clinical review.
Does coeliac disease always cause weight loss along with bloating?
Not always; many individuals with coeliac disease maintain a stable weight but experience persistent bloating and nutrient deficiencies as their primary symptoms.
What does a CA125 blood test check for?
CA125 is a protein marker in the blood that can be elevated in various conditions, and it is used as an initial screen for ovarian health in women with persistent bloating.
Can constipation cause the same type of bloating as IBS?
Yes, constipation is a major cause of bloating because trapped waste prevents gas from passing, leading to significant abdominal pressure and swelling.
Authority Snapshot (E-E-A-T)
This medical content is designed to provide evidence-based educational information for the UK public regarding digestive and abdominal health. The material is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with extensive experience across internal medicine, general surgery, and acute care. All information provided is strictly aligned with the clinical standards and diagnostic pathways set by the NHS and the National Institute for Health and Care Excellence (NICE).


