

An anal fissure is a common condition that often improves with conservative home care, but specific symptoms or persistent discomfort require a formal clinical assessment to ensure an accurate diagnosis. A fissure is a small tear in the lining of the anal canal that can cause significant pain and bleeding, often mirroring the symptoms of other gastrointestinal conditions. In the United Kingdom, healthcare professionals follow structured diagnostic pathways to differentiate benign fissures from more complex issues such as inflammatory bowel disease. Knowing the indicators for a medical review helps patients receive appropriate treatment early, preventing acute injuries from developing into chronic, non-healing wounds that impact long-term quality of life.
What We’ll Discuss in This Article
- Indicators for seeking a routine appointment with a GP
- Recognising red flag symptoms that require prioritised review
- The importance of assessing rectal bleeding and bowel changes
- Distinguishing between acute pain and signs of infection
- How clinical investigations are used to confirm a diagnosis
- National standards for referral to specialist colorectal services
General Indicators for a Routine Clinical Review
You should see a doctor about an anal fissure if your symptoms do not show significant improvement after two weeks of following healthy lifestyle habits and using over-the-counter treatments. While many minor tears heal spontaneously once constipation is managed and stools are kept soft, a persistent fissure indicates that the underlying cycle of muscle spasm and restricted blood flow remains unresolved. An anal fissure is a small tear in the moist, thin tissue that lines the anus, and it can usually be managed with simple treatments if it is identified early.
If the sharp, stinging pain during bowel movements continues to disrupt your daily routine, a GP can perform a gentle examination to confirm the presence of the tear. A clinical review allows for the prescription of specific medicated ointments, such as calcium channel blockers or nitrates, which are more effective than standard soothing creams at relaxing the anal sphincter. Early intervention is particularly important to prevent the tissue from developing the thickened edges and skin tags characteristic of a chronic fissure, which can be significantly more difficult to treat without specialist help.
Evaluating Rectal Bleeding and Its Characteristics
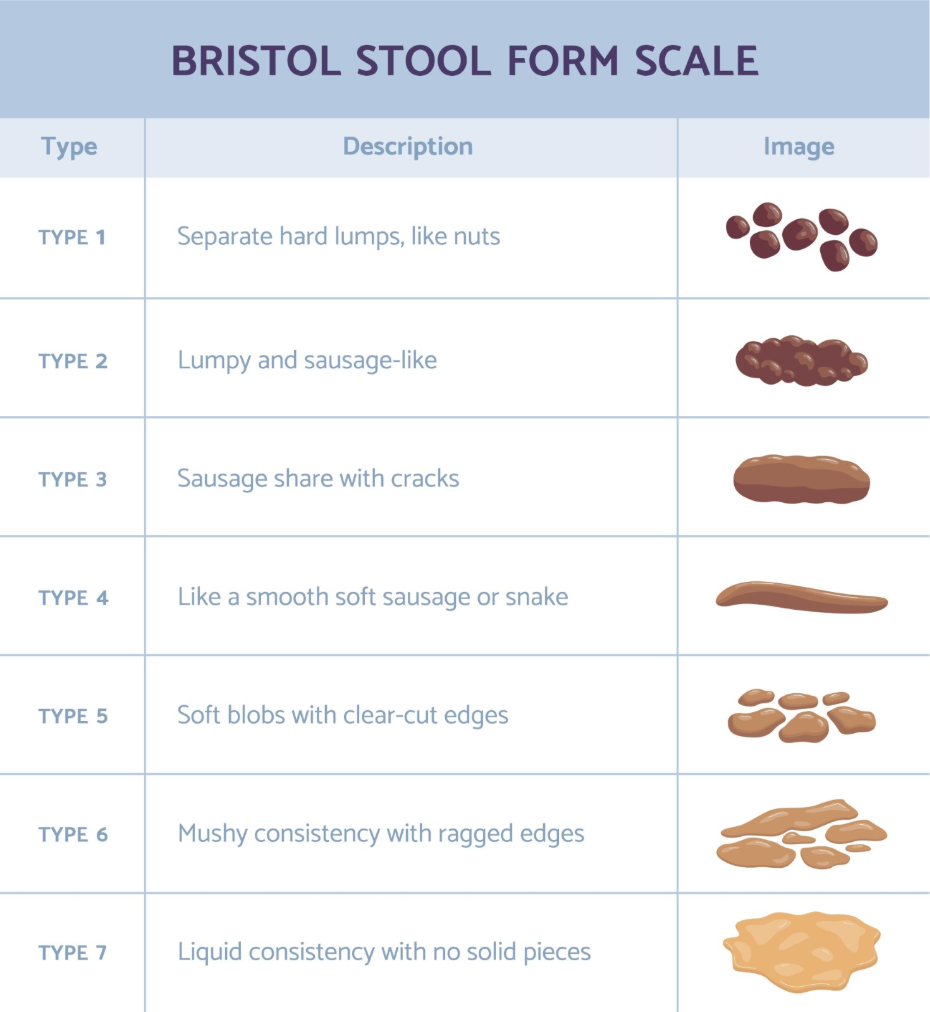
Rectal bleeding is a primary reason to seek medical advice, as any instance of passing blood must be professionally evaluated to determine its exact source. In the context of an anal fissure, bleeding is typically bright red and noticed in small amounts on the toilet tissue or the surface of the stool. The symptoms of an anal fissure often include a sharp pain when you go to the toilet and bright red blood on your poo or the toilet paper.
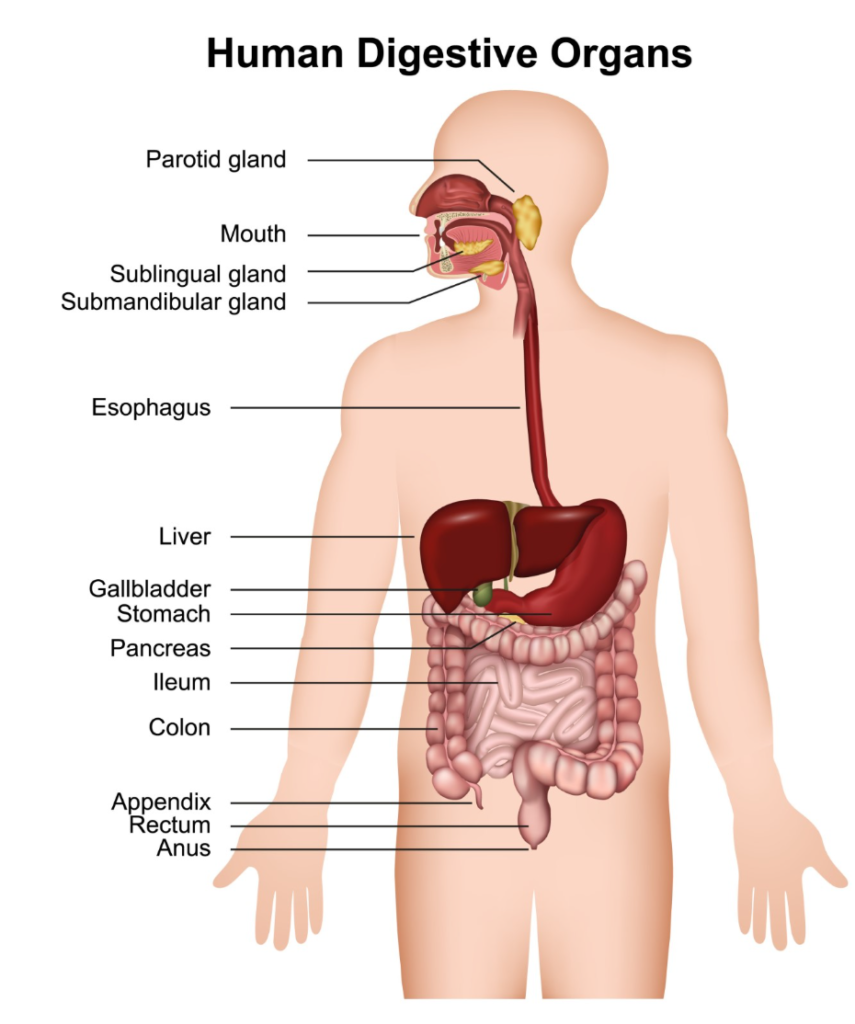
While this pattern is common for fissures, a clinician must rule out other causes of bleeding higher up in the digestive tract. You should seek a prioritised medical review if the bleeding is heavy, dark in colour, or mixed within the stool itself. National clinical guidelines provide structured advice for clinicians to investigate rectal bleeding, ensuring that symptoms are investigated according to the patient’s age and clinical history. Providing a clear description of the blood’s appearance and whether it is accompanied by pain helps the healthcare provider decide which diagnostic tests are necessary to ensure the digestive system is functioning correctly.
Changes in Bowel Habits and Systemic Symptoms
A medical review is essential if anal pain is accompanied by a persistent change in bowel habits or other systemic symptoms that could indicate an underlying condition. If you notice that your bowel movements have become more frequent, looser, or more difficult to pass for a period of three weeks or more, this change warrants investigation. These symptoms, when paired with an anal fissure, might suggest that the tear is secondary to a broader issue such as Crohn’s disease or ulcerative colitis.
Healthcare professionals also look for “red flag” symptoms that suggest a need for more comprehensive screening. These include unintentional weight loss, persistent abdominal pain, or a feeling of incomplete emptying after using the toilet. When you consult a GP about anal discomfort, they will ask about these factors to determine if a simple fissure is the primary issue or if a referral for further tests, such as a colonoscopy or blood tests, is required. Monitoring these changes helps ensure that management plans are strictly aligned with national health standards and patient safety protocols.
Signs of Infection and Acute Complications
The development of signs suggesting a local infection or an abscess near the site of an anal fissure requires an urgent clinical assessment. While a fissure is a simple skin tear, the location makes it susceptible to bacteria, which can lead to a localised infection or the formation of a perianal abscess. If the sharp pain of a fissure transitions into a constant, throbbing ache that is not relieved by warm soaks, it may indicate that an infection is developing in the deeper tissues.
You should seek prompt medical advice if you experience:
- A fever or chills accompanied by anal pain
- Pus-like discharge from the anal opening or the site of the tear
- A hard, hot, or increasingly painful lump near the anus
- Redness and swelling that spreads to the surrounding skin
- Severe pain that prevents you from sitting, walking, or passing stool
An abscess requires specific clinical management, such as drainage and potentially antibiotics, which differ significantly from standard fissure treatments. Identifying these complications early prevents the development of more complex issues, such as an anal fistula, which is a small tunnel that develops between the end of the bowel and the skin.
Diagnostic Procedures in Primary Care
When you see a doctor for a suspected anal fissure, they will follow a systematic diagnostic process to confirm the diagnosis while minimising your discomfort. This typically begins with a detailed review of your medical history, focusing on your bowel habits and any previous gastrointestinal issues. A physical examination is usually required, which often involves a gentle visual inspection of the anal margin while you lie on your side with your knees drawn up.
In many cases, a visual check is sufficient to see the tear, especially if it is located at the posterior midline. A digital rectal examination, where the clinician uses a lubricated, gloved finger to check the internal rectum, may be deferred if the pain is too severe, as this could cause further trauma to the fissure. If the diagnosis remains unclear, or if there is a need to rule out other issues, a GP may use a proctoscope (a small hollow tube with a light) to look at the anal canal once the initial pain has been managed with medication.
Comparison of Symptom Categories and Referral Urgency
The following table summarises when different symptoms transition from routine management to requiring prioritised clinical attention.
| Symptom Category | Routine Review (2 weeks) | Prioritised Review (Persistent/Severe) |
| Anal Pain | Sharp sting only when pooing | Constant throbbing or prevents sleep |
| Bleeding | Small streaks of bright red blood | Heavy, dark, or mixed with the stool |
| Visible Sign | Small shallow tear or crack | Hard, hot lump or pus-like discharge |
| Bowel Habits | Temporary constipation | Change lasting 3 weeks or more |
| General Health | No other symptoms | Weight loss or severe abdominal pain |
Conclusion
Most anal fissures improve with home care, but a medical review is necessary if symptoms persist for more than two weeks or if you experience red flag signs like heavy bleeding or fever. A GP can provide an accurate diagnosis and access to medicated treatments that help the anal muscles relax and support healing. Following national clinical standards ensures that any rectal discomfort is investigated thoroughly to exclude other underlying conditions. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can a pharmacist help with an anal fissure?
Yes, UK pharmacists can provide advice on over-the-counter soothing treatments and help you decide if your symptoms require a GP appointment.
Should I see a doctor if I only have blood but no pain?
Painless rectal bleeding is more common with internal haemorrhoids, but it still requires a professional medical review to confirm the source.
What is the “three-week rule” for bowel habits?
In the UK, any unexplained change in bowel habits lasting three weeks or more should be reported to a GP for investigation.
Will the doctor need to do a colonoscopy for a fissure?
A colonoscopy is usually not needed for a simple fissure, but it may be offered if there are other symptoms or if you are over a certain age.
Can I see a doctor if I am too embarrassed for an exam?
Healthcare professionals perform these examinations routinely and will ensure your privacy and comfort; a diagnosis is essential for the correct treatment.
Is an anal fissure ever an emergency?
A simple fissure is not an emergency, but severe pain accompanied by fever or a hot, hard lump requires urgent assessment for a possible abscess.
What should I bring to my appointment?
It is helpful to have a record of your symptoms, including when they started, the appearance of any blood, and any changes in your stool consistency.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the clinical management of anal fissures for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
