An anal fissure is diagnosed through a combination of a detailed review of a patient’s medical history and a gentle physical examination of the anal area. Healthcare professionals in the United Kingdom follow structured protocols to confirm the presence of a tear while ensuring that other potential causes of rectal pain and bleeding are ruled out. Because an anal fissure is essentially a visible injury to the lining of the anal canal, a diagnosis can often be made during a routine consultation with a General Practitioner or a specialist. Understanding the diagnostic process helps to alleviate concerns about the examination and ensures that the correct management strategy is initiated to support tissue healing and muscle relaxation.
What We’ll Discuss in This Article
- The initial clinical consultation and symptom assessment
- Physical examination techniques including visual inspection
- The role of a digital rectal examination in diagnosis
- Specialised internal investigations such as proctoscopy
- Differentiating fissures from other conditions like haemorrhoids
- Diagnostic pathways for chronic or non-healing fissures
- When further hospital-based investigations may be required
Initial Clinical Consultation and History Taking
The diagnostic process begins with a structured conversation where the clinician gathers detailed information about the nature, timing, and duration of the symptoms. A healthcare professional will ask specific questions regarding the type of pain experienced, focusing on whether it is a sharp, stinging sensation that occurs during bowel movements and if a throbbing ache persists afterwards. They will also explore the characteristics of any rectal bleeding, such as whether bright red blood is noticed on the toilet paper or the surface of the stool.
In addition to symptom review, the clinician will assess the patient’s bowel habits and lifestyle factors. An anal fissure is a small tear in the moist, thin tissue (mucosa) that lines the anus, and it is most commonly caused by constipation or the passage of hard, large stools. By discussing dietary fibre intake, hydration levels, and any history of straining, the doctor can identify the likely mechanical cause of the tear. This history-taking phase is essential for determining if the fissure is an acute injury or if it has become a chronic condition that requires specific medical intervention.
Visual Inspection and External Assessment
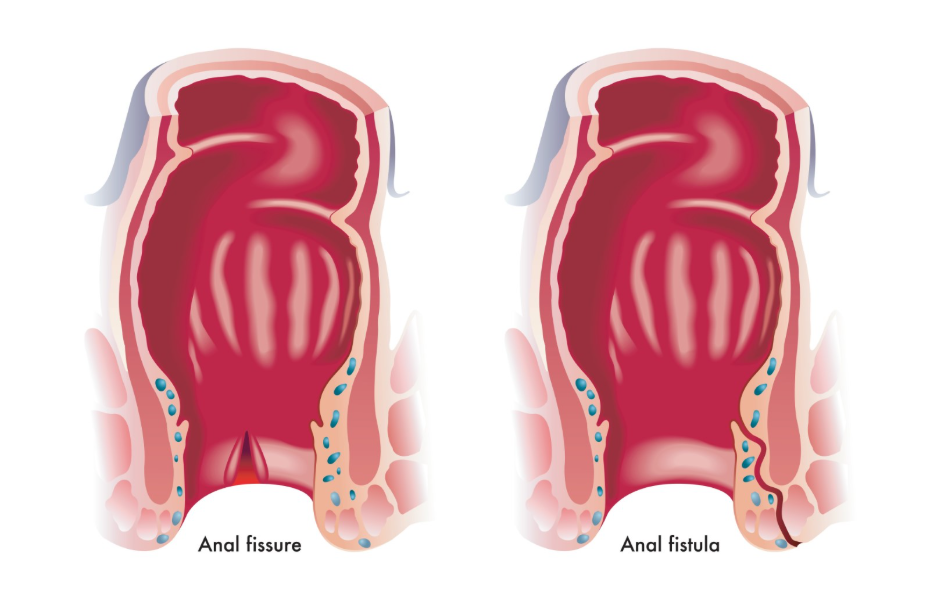
A visual inspection of the perianal area is the primary method used to confirm the presence of an anal fissure. During this part of the examination, the patient is typically asked to lie on their side with their knees drawn up toward their chest in a private clinical setting. The healthcare professional will gently separate the buttocks to look for a small, linear crack or split in the skin at the anal opening.
In acute cases, the fissure may look like a fresh paper cut. If the fissure has been present for longer than six weeks, the clinician may observe structural changes, such as thickened edges around the tear or a small skin tag known as a sentinel pile. The National Institute for Health and Care Excellence provides guidelines for the management of anal fissures, noting that a diagnosis can often be made by simple visual inspection of the anal margin. A visual assessment is often sufficient for a diagnosis, especially when the characteristic sharp pain makes a more invasive internal examination difficult during the initial visit.
The Digital Rectal Examination
A digital rectal examination is a standard diagnostic procedure used to assess the health of the rectum and the tension of the anal sphincter muscles. After putting on a lubricated glove, the clinician gently inserts a finger into the anal canal to feel for abnormalities or lumps. This test helps to determine the resting tone of the internal anal sphincter, as a high resting pressure or muscle spasm is a common feature of a non-healing anal fissure.
However, if the patient is in significant pain, a clinician may decide to defer the digital rectal examination until the initial pain has been managed with medication or warm soaks. This is because the act of inserting a finger can be acutely painful and may cause further trauma to the tear. When performed, the examination allows the doctor to rule out other conditions such as internal haemorrhoids or polyps. The findings from this procedure are vital for deciding whether the patient requires specific medicated ointments designed to relax the anal muscles and improve blood flow to the site of the injury.
Proctoscopy and Internal Visualisation
A proctoscopy is a simple diagnostic test used to view the lining of the anal canal and the lower rectum using a small, hollow tube called a proctoscope. This instrument is lubricated and gently inserted, allowing the clinician to inspect the internal mucosal surface under direct light. While a fissure is often visible externally, a proctoscopy can help identify if the tear extends further into the canal or if there are multiple fissures present.
This procedure is typically performed in a GP surgery or an outpatient clinic and does not usually require sedation. It is particularly useful for distinguishing a fissure from internal haemorrhoids, as both can cause bright red bleeding. By visualising the internal cushions, the clinician can ensure that the management plan is tailored to the correct condition. If a proctoscopy is too uncomfortable during the first consultation, it may be scheduled for a follow-up appointment once the acute inflammation has subsided.
Differentiating Fissures from Other Conditions
Differentiating an anal fissure from other common anorectal conditions is a critical part of the diagnostic process. While the symptoms may overlap, the physical findings and the nature of the pain help the clinician make an accurate identification.
| Feature | Anal Fissure | Haemorrhoids (Piles) |
| Primary Pain | Sharp, cutting, or stinging | Dull ache or throbbing |
| Pain Timing | During and shortly after pooing | Can be constant or unrelated to poo |
| Bleeding | Bright red, linked to sharp pain | Bright red, often painless |
| Physical Sign | A visible crack or tear in the skin | Soft lumps or swollen veins |
| Muscle Spasm | Common and causes throbbing | Rare |
If the diagnosis is not entirely clear, or if there are atypical features such as a fissure located away from the midline, the clinician may consider other underlying causes. These can include inflammatory bowel disease, such as Crohn’s disease, or certain infections. Identifying these distinctions ensures that the patient receives the appropriate specialist care if the fissure is a secondary symptom of a broader health issue.
Diagnostic Pathways for Chronic Fissures
When a fissure fails to heal within six weeks, healthcare professionals follow a specific pathway to manage it as a chronic condition. A chronic fissure often shows physical signs of long-term inflammation, such as the exposure of the underlying sphincter muscle fibres at the base of the wound. The diagnosis of a chronic fissure is as much about the time it has persisted as it is about its physical appearance.
Clinicians will assess why the healing process has stalled, often focusing on the role of muscle spasms. Chronic anal fissures may require a referral to a specialist if they do not respond to initial treatments like glyceryl trinitrate (GTN) or diltiazem cream. A specialist review may involve more detailed assessments of the pelvic floor and the anal sphincter’s function. In some cases, the diagnosis of a chronic fissure is the starting point for discussing more advanced management options, such as botulinum toxin injections or minor surgical procedures to reduce muscle tension.
When Further Investigations Are Needed
Further hospital-based investigations are typically reserved for cases where the diagnosis is uncertain, symptoms are severe, or there are “red flag” indicators. If a patient experiences significant rectal bleeding, unintentional weight loss, or a persistent change in bowel habits, a clinician may refer them for a colonoscopy or a sigmoidoscopy. These procedures use a flexible camera to examine the entire colon or the lower part of the large intestine.
These investigations are essential for ruling out conditions like colorectal cancer or significant inflammatory bowel disease, especially in older adults or those with a family history of such conditions. While a simple anal fissure is the most likely cause of sharp pain, national clinical standards in the UK ensure that all rectal symptoms are investigated thoroughly. By following these established diagnostic steps, healthcare providers ensure that every patient receives a safe, accurate diagnosis and an effective treatment plan.
Conclusion
Anal fissures are diagnosed through a careful review of symptoms and a gentle physical examination, including visual inspection and sometimes a digital rectal exam. While the sharp pain can make the process daunting, clinicians are trained to perform these checks with minimal discomfort. Establishing whether a fissure is acute or chronic is vital for choosing the correct medicated treatments to support healing. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is the examination for a fissure painful?
A visual inspection is usually not painful, although a digital rectal exam may be slightly uncomfortable or deferred if the pain from the tear is currently too severe.
Can a GP diagnose a fissure or do I need a specialist?
Most anal fissures are diagnosed and managed by a GP; a specialist referral is usually only needed if the fissure becomes chronic or does not heal.
Will I need a camera test for a fissure?
A camera test like a colonoscopy is generally not needed for a simple fissure unless there are other symptoms or a need to rule out different conditions.
What is the difference between a proctoscopy and a digital exam?
A digital exam uses a finger to feel the rectum, whereas a proctoscopy uses a small tube and light to see the lining of the anal canal directly.
How do I prepare for the examination?
No special preparation is needed; you do not need to fast or use an enema before a routine examination for an anal fissure.
Can a fissure be diagnosed without a physical exam?
While symptoms provide a strong indication, a physical exam is necessary to confirm the diagnosis and ensure the symptoms are not caused by something else.
What should I tell my doctor before the exam?
Inform your doctor about the exact type of pain you feel, the colour of any blood you have seen, and your recent bowel habits.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the diagnosis of anal fissures for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
