Treatments for anal fissures focus on relaxing the anal sphincter muscle and softening the stool to allow the delicate lining of the anal canal to heal naturally. An anal fissure is a small tear in the moist tissue that lines the anus, often caused by constipation or physical strain, resulting in intense pain and bright red bleeding. While many acute fissures resolve with conservative home care, persistent or chronic cases may require specifically medicated ointments or clinical procedures to break the cycle of muscle spasm and restricted blood flow. In the United Kingdom, healthcare professionals follow a structured treatment pathway that prioritises non-invasive measures before considering surgical interventions, ensuring that each patient receives care appropriate to the severity of their symptoms.
What We’ll Discuss in This Article
- Conservative management through dietary and lifestyle changes
- The use of fibre supplements and laxatives to improve stool consistency
- Topical medications and muscle relaxants for pain and healing
- Specialised clinical treatments for chronic anal fissures
- Surgical options for cases resistant to conservative care
- National clinical standards for the management of anal tears
Conservative Management and Lifestyle Changes
Conservative management is the first-line treatment for anal fissures and focuses on ensuring that stools remain soft and easy to pass without the need for straining. The mechanical trauma of passing hard stools is the primary reason why fissures occur and why they often struggle to heal. By making specific adjustments to diet and daily habits, individuals can reduce the friction placed on the anal canal, allowing the body’s natural repair mechanisms to function effectively.
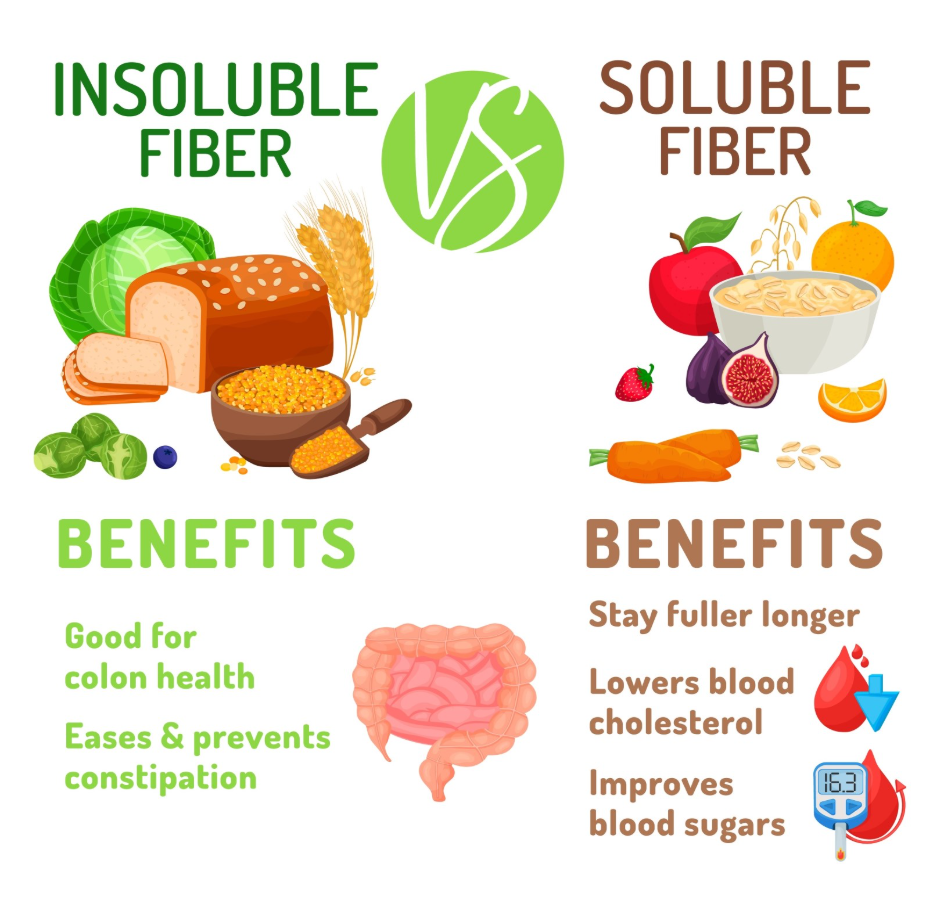
Anal fissures are small tears in the lining of the anus, and they often get better within a few weeks if you take steps to keep your poo soft, such as increasing the amount of fibre in your diet. Patients are encouraged to aim for the UK daily target of 30g of fibre from sources such as whole grains, pulses, fruits, and vegetables. This must be accompanied by adequate hydration, as fibre requires water to keep the waste material pliable. Warm sitz baths (soaking the area in plain warm water) are also recommended several times a day to help the anal muscles relax and improve local blood flow, which is vital for tissue repair.
Fibre Supplements and Stool Softeners
If dietary changes alone are insufficient to achieve a soft stool consistency, healthcare professionals may recommend the use of bulk-forming laxatives or stool softeners. These supplements work by increasing the amount of water the stool retains, making it bulkier and more lubricated. This ensures that the anal canal does not have to stretch excessively during a bowel movement, which prevents the healing tear from being re-opened.
The National Institute for Health and Care Excellence provides guidelines on the use of laxatives for managing constipation in patients with anal fissures to reduce the pain associated with passing stool. Bulk-forming laxatives, such as ispaghula husk, are typically preferred as they mimic the action of dietary fibre. It is essential to drink plenty of fluids when using these supplements to avoid a potential worsening of constipation. These aids are usually used for a few weeks until the fissure has shown significant signs of healing and a consistent bowel routine has been established.
Medicated Ointments and Muscle Relaxants
For fissures that do not heal with simple lifestyle changes, specifically medicated ointments are used to relax the internal anal sphincter muscle and improve blood circulation to the wound. Chronic fissures often enter a cycle where the pain causes the muscle to go into a spasm, which then restricts the blood supply needed for the skin to knit back together. These specialised ointments work by chemically reducing the resting pressure of the anal canal.
In the UK, two common types of medicated ointments are used:
- Glyceryl Trinitrate (GTN): This ointment releases nitric oxide, which causes the smooth muscle of the anal sphincter to relax and improves local perfusion.
- Calcium Channel Blockers: Medications such as diltiazem or nifedipine are often used as an alternative, blocking calcium entry into muscle cells to reduce tension with a lower risk of side effects like headaches.
Anal fissures that do not heal within a few weeks may be treated with glyceryl trinitrate (GTN) ointment to help the anal muscles relax and increase blood flow to the area. These treatments are usually applied twice daily for six to eight weeks. They are highly effective at breaking the cycle of pain and spasm, provided they are used consistently alongside a high-fibre diet.
Specialised Clinical Treatments for Chronic Fissures
If topical medications do not resolve a chronic fissure, more advanced clinical treatments such as botulinum toxin injections may be considered. This procedure involves injecting the toxin directly into the anal sphincter muscle to temporarily paralyse it. The paralysis lasts for several months, which ensures the muscle remains relaxed and allows the fissure to heal undisturbed by spasms or high pressure.
This treatment is typically performed in a specialist outpatient clinic or a hospital setting. While effective, it carries a small risk of temporary minor incontinence to gas or stool, which the clinician will discuss during the consultation. Botulinum toxin is generally reserved for cases where topical treatments have failed or cannot be tolerated. It serves as a middle-ground option before more permanent surgical changes to the anal sphincter are discussed.
Surgical Options for Resistant Fissures
Surgery is generally considered only when all other treatment options have failed to heal a chronic anal fissure. The most common surgical procedure in the UK is a lateral internal sphincterotomy. This involves making a small cut in the internal anal sphincter muscle to permanently reduce its resting tension. By lowering the internal pressure of the anal canal, the blood flow is restored, and the fissure is finally able to heal.
| Procedure | Description | Success Rate | Recovery Time |
| Sphincterotomy | A small cut in the anal muscle | Very High | 2 to 4 weeks |
| Anal Advancement Flap | Using healthy skin to cover the tear | Moderate to High | 3 to 6 weeks |
An anal advancement flap is an alternative surgical method where a piece of healthy skin from another part of the anal area is moved to cover the fissure. This is sometimes preferred if there is a higher risk of incontinence from a sphincterotomy. While surgery is highly successful in preventing the recurrence of fissures, it involves risks such as infection or long-term changes in bowel control, which require careful consideration and discussion with a consultant surgeon.
Comparing Treatment Categories
The table below distinguishes the different levels of treatment based on the chronicity of the anal tear.
| Treatment Category | Primary Goal | Typical Duration |
| Conservative | Soften stool and soothe skin | 2 to 4 weeks |
| Topical Medicated | Relax muscle and boost blood flow | 6 to 8 weeks |
| Advanced Clinical | Temporary muscle paralysis | 3 to 6 months (effect) |
| Surgical | Permanent muscle relaxation | Lifetime (structural change) |
Conclusion
Anal fissure treatments range from simple dietary changes and warm soaks to medicated ointments and, in rare cases, surgery. Most acute fissures resolve with a focus on high fibre and hydration, which prevents the mechanical trauma that keeps the tear open. Chronic cases require interventions that specifically target the anal sphincter muscle to restore blood flow and break the cycle of pain. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can I get fissure treatment over the counter?
Soothing creams and fibre supplements are available over the counter, but muscle relaxants like GTN or diltiazem require a prescription from a GP.
How long do I need to use the medicated cream?
Most clinical protocols recommend using medicated ointments for six to eight weeks to ensure the tissue has completely healed and stabilised.
Why does my fissure hurt again after it started healing?
Recurrence often happens if you become constipated again, as a hard stool can easily re-tear the fragile new skin cells.
Is surgery for anal fissures common?
No, surgery is only considered for a small percentage of patients whose fissures do not respond to multiple rounds of non-invasive treatment.
Does a sitz bath really help with healing?
Yes, soaking in warm water helps the anal sphincter relax and improves local circulation, which are both essential for the healing process.
Are there side effects to the medicated ointments?
GTN can cause headaches due to its effect on blood vessels, while calcium channel blockers have a lower risk of this specific side effect.
Can I have treatment if I am pregnant?
Management during pregnancy focuses on conservative care; you should consult your midwife or GP before using any medicated ointments.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the treatment options for anal fissures for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
