

Haemorrhoids and anal fissures are common anorectal conditions that often arise from mechanical factors, yet they may also be associated with wider medical issues. While many cases are isolated incidents related to lifestyle, some instances serve as clinical indicators of underlying digestive or systemic conditions. Understanding these associations helps in identifying when a local symptom might be part of a broader health picture requiring professional investigation. Clinical pathways in the United Kingdom focus on treating the immediate symptoms while considering whether an underlying pathology, such as chronic inflammation or vascular pressure, is contributing to the persistence of these issues.
What We’ll Discuss in This Article
- The relationship between chronic constipation and digestive disorders
- Associations between anal fissures and inflammatory bowel disease
- How pregnancy and hormonal changes impact rectal health
- Links between liver health and the development of haemorrhoids
- The impact of systemic inflammatory conditions on the anal lining
- Clinical diagnostic pathways for ruling out associated conditions
Digestive Health and Chronic Constipation
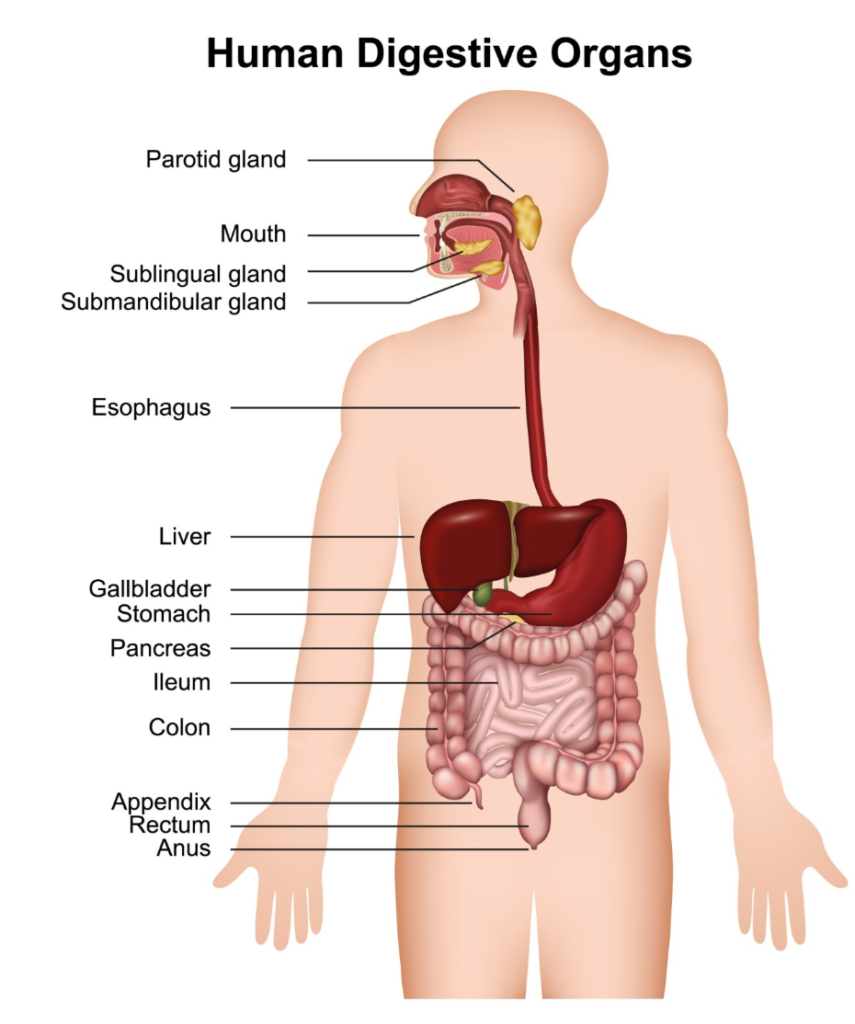
Chronic digestive issues such as constipation are the most significant medical factors associated with both haemorrhoids and anal fissures. When the digestive system slows down, the stool remains in the colon longer, where the body reabsorbs water, resulting in hard and dry waste. The effort required to expel this waste creates significant mechanical stress on the anal canal, leading to the formation of tears or the swelling of rectal veins.
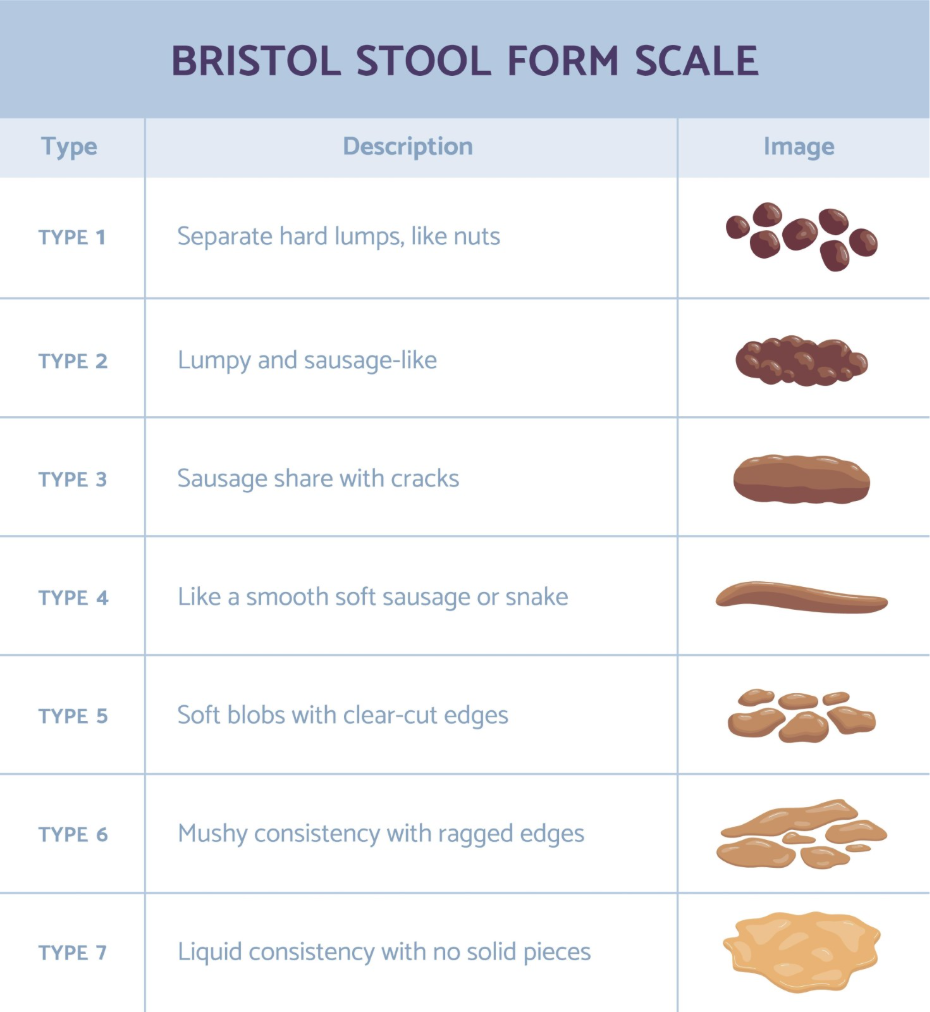
Haemorrhoids are swollen veins in the anus and lower rectum that are frequently caused by chronic constipation and straining during bowel movements. This relationship is circular, as the presence of a fissure or painful haemorrhoid can cause a person to subconsciously delay using the toilet, which further worsens constipation. Over time, chronic constipation may be a symptom of functional bowel disorders such as irritable bowel syndrome (IBS). In these cases, the anorectal issues are often managed as a secondary symptom of the primary digestive transit problem.
Inflammatory Bowel Disease (IBD)
Anal fissures, particularly those that are recurrent or found in unusual locations, can be a clinical sign of inflammatory bowel diseases such as Crohn’s disease or ulcerative colitis. Unlike standard fissures caused by constipation, which usually occur at the front or back of the anal opening, fissures associated with IBD may appear at the sides or occur in multiples. This is because the chronic inflammation associated with IBD can thin the mucosal lining and make it more fragile.
The National Institute for Health and Care Excellence notes that while most anal fissures are simple tears, they can sometimes be associated with underlying conditions like Crohn’s disease. In patients with Crohn’s disease, the inflammation can penetrate deep into the tissues of the anal canal, leading to complications like skin tags or fistulas alongside the fissure. If a fissure fails to heal with standard treatments or is accompanied by symptoms like persistent diarrhoea, abdominal pain, or weight loss, health professionals will often investigate for underlying inflammatory conditions.
Pregnancy and Pelvic Health
Pregnancy is a physiological state frequently associated with the development of both haemorrhoids and anal fissures due to increased pelvic pressure and hormonal shifts. As the uterus expands, it puts direct pressure on the pelvic veins and the inferior vena cava, which can cause blood to pool in the rectal vessels. This venous congestion is a primary driver for the development of haemorrhoids during the second and third trimesters.
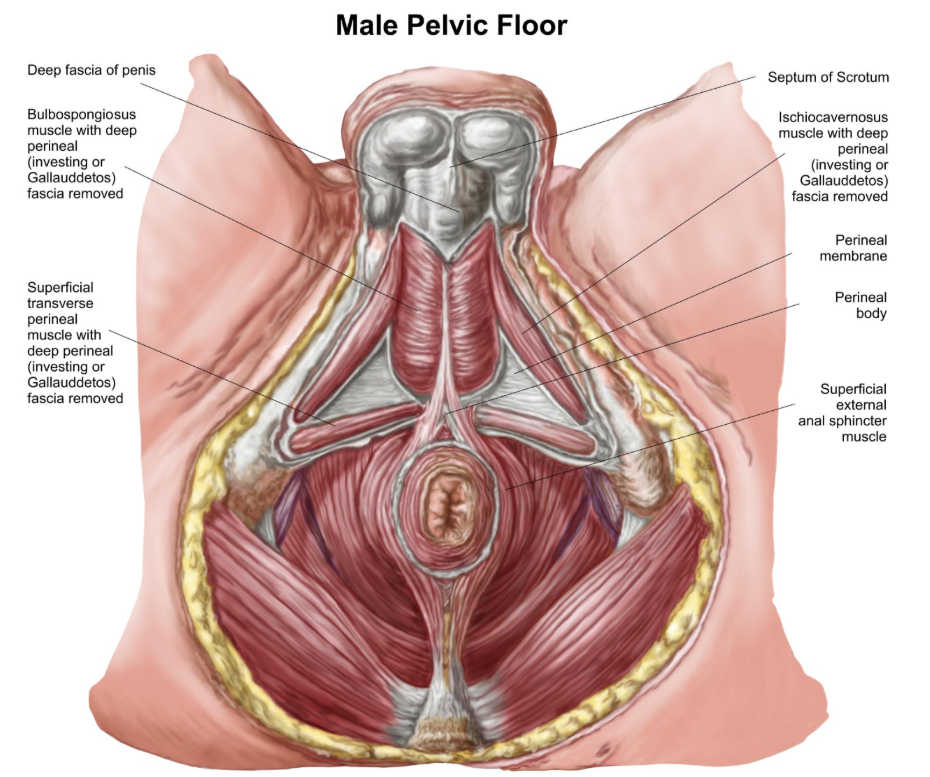
Additionally, the hormone progesterone, which increases significantly during pregnancy, has a relaxing effect on the smooth muscles of the digestive tract. This relaxation slows down gut motility, making constipation much more likely. The combination of slower digestion and increased physical pressure creates a high risk environment for both skin tears and vascular swelling. While these issues often resolve after childbirth, they are managed carefully during pregnancy to ensure comfort and to prevent long term changes to the pelvic floor muscles.
Liver Disease and Portal Hypertension
Haemorrhoids can occasionally be linked to chronic liver conditions that cause increased pressure in the portal venous system. The portal vein carries blood from the digestive organs to the liver; if the liver is scarred or damaged, blood cannot flow through it easily, causing pressure to build up in the connected veins. This condition, known as portal hypertension, can lead to the formation of varices, which are swollen veins in the oesophagus or the rectum.
While most haemorrhoids are caused by local pressure from straining, anorectal varices caused by liver disease can mimic the appearance of haemorrhoids. It is important to distinguish between the two, as management for varices focuses on reducing systemic venous pressure rather than just local treatment. Clinicians may look for other signs of liver health, such as jaundice or abdominal swelling, when assessing patients with severe or unusual vascular swelling in the rectal area.
Systemic Conditions and Immune Health
Certain systemic conditions that affect the immune system or cause widespread inflammation can contribute to the fragility of the anal lining and the risk of fissures. Conditions that suppress the immune response can make it difficult for the body to repair minor tears in the anal mucosa, potentially turning an acute fissure into a chronic wound. Furthermore, certain infections can manifest with symptoms that are very similar to a standard anal fissure.
An anal fissure is a small tear in the lining of the anus that can sometimes be related to more complex medical issues or infections. When an anal injury occurs in the context of a compromised immune system, the healing process is often prolonged because the body cannot effectively manage the local bacterial environment. In these instances, the management strategy focuses on both the local injury and the underlying systemic health of the patient.
Comparison of Associated Medical Factors
The following table provides a comparison of how different medical conditions interact with the anal canal and the rectum.
| Condition | Primary Impact on Rectal Area | Most Common Association |
| Chronic Constipation | Mechanical trauma and straining | Both fissures and haemorrhoids |
| Crohn’s Disease | Deep tissue inflammation and ulceration | Recurrent or multiple fissures |
| Pregnancy | Increased venous pressure and slow transit | Haemorrhoids and acute tears |
| Liver Disease | Portal venous hypertension | Anorectal varices (piles) |
| IBS | Irregular bowel movements (diarrhoea/constipation) | Both conditions |
Conclusion
Haemorrhoids and anal fissures are frequently linked to digestive health issues like chronic constipation, but they can also be indicators of inflammatory bowel disease or liver conditions. Physical states such as pregnancy are also well known triggers due to the increased pressure they place on the pelvic floor. Recognising these links ensures that symptoms are not just treated in isolation but are understood as part of a person’s overall health. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can IBS cause anal fissures?
Yes, the irregular bowel habits associated with IBS, particularly constipation or frequent diarrhoea, can irritate the anal lining and cause tears.
Is there a link between haemorrhoids and heart disease?
There is no direct link, but both conditions share lifestyle risk factors such as a low fibre diet and a sedentary lifestyle.
Why does Crohn’s disease cause fissures?
Crohn’s disease causes inflammation throughout the digestive tract, which makes the mucosal lining thin and more likely to split.
Can haemorrhoids be a sign of liver problems?
In some cases, severe rectal swelling can be a sign of portal hypertension related to chronic liver issues, though this is less common than standard piles.
Do fissures heal slower if I have other conditions?
Yes, conditions like diabetes or IBD can slow down the body’s natural repair mechanisms, making a fissure more likely to become chronic.
Are children with fissures likely to have other conditions?
In children, fissures are almost always related to simple constipation and toilet avoidance rather than underlying systemic diseases.
Can anaemia be caused by haemorrhoids?
If haemorrhoids bleed heavily and persistently over a long period, it can potentially lead to iron deficiency anaemia.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence based information for the UK public regarding the associations between anorectal issues and other health conditions. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK trained physician with experience in general surgery, emergency care, and clinical education. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
