

An anal fissure that is left managed incorrectly or left entirely untreated can lead to a range of clinical complications, most notably the transition from an acute injury to a chronic, non-healing wound. While many small tears in the anal lining resolve within a few weeks with simple dietary adjustments, those that persist can cause structural changes to the anal canal and significant daily distress. Chronic fissures are often characterised by a cycle of pain and muscle tension that restricts the blood flow necessary for natural tissue repair. Understanding the potential for long term issues, such as the development of skin tags or the risk of localised infection, is essential for patients navigating the recovery process within the UK health system.
What We’ll Discuss in This Article
- The progression from acute to chronic anal fissures
- Development of sentinel piles and internal structural changes
- The impact of persistent muscle spasms and restricted blood flow
- Risk of infection, perianal abscesses, and anal fistulas
- Permanent scarring and the potential for anal stenosis
- The importance of breaking the cycle of pain and constipation
The Progression to Chronic Anal Fissures
An anal fissure that is left untreated for longer than six weeks is classified as chronic, often requiring more intensive medical management than a fresh tear. Most acute fissures look like a simple, shallow cut in the lining of the anal canal, similar to a paper cut on the skin. However, when the tear fails to heal because of repeated trauma or lack of intervention, it deepens and begins to involve the underlying muscle fibres.
An anal fissure is a small tear in the lining of the anus, and if it does not heal within six weeks, it is considered a chronic fissure. In a chronic state, the body’s inflammatory response remains active, but the regenerative process is stalled. The edges of the fissure may become thickened and raised, making it increasingly difficult for the skin to knit back together naturally. This transition marks a shift in clinical approach, as chronic fissures are significantly less likely to resolve with fibre and water alone, often necessitating the use of specifically medicated ointments to facilitate healing.
Development of Sentinel Piles and Structural Changes
Untreated fissures can lead to the formation of physical structural changes around the anal opening, such as sentinel piles or anal papillae. As a fissure remains open for an extended period, the chronic inflammation causes the surrounding skin to thicken and produce excess tissue. A sentinel pile, also known as a sentinel tag, is a small skin tag that develops at the base of the fissure, often appearing as a small lump near the anus.
Internally, at the top of the tear, a similar growth called a hypertrophied anal papilla may form. While these structures are benign, they can cause additional discomfort, itching, and difficulty maintaining hygiene in the perianal area. These structural markers are clinical signs that a fissure has been present for a significant amount of time. If the original tear is not managed, these tags can become large enough to cause irritation during physical activity or interfere with the ease of bowel movements.
Impact of Persistent Sphincter Spasms
The persistent sharp pain from an untreated fissure often triggers involuntary spasms of the anal sphincter muscle, which further restricts blood flow to the injury site. The internal anal sphincter is a ring of muscle that remains under involuntary control, and its primary job is to keep the anal canal closed. When a fissure is present, the exposure of sensitive nerves to the environment causes the muscle to contract sharply as a protective reflex.
This spasm is a major complication because it leads to a condition known as ischaemia, or restricted blood supply. The blood vessels that supply the anal lining must pass through the sphincter muscle; when the muscle is in constant spasm, it compresses these vessels. The National Institute for Health and Care Excellence provides structured guidance for managing fissures that fail to respond to conservative care to prevent long term complications. Without adequate blood flow, the oxygen and nutrients required for tissue repair cannot reach the tear, effectively trapping the patient in a cycle of pain, spasm, and non-healing.
Risk of Infection and Abscess Development
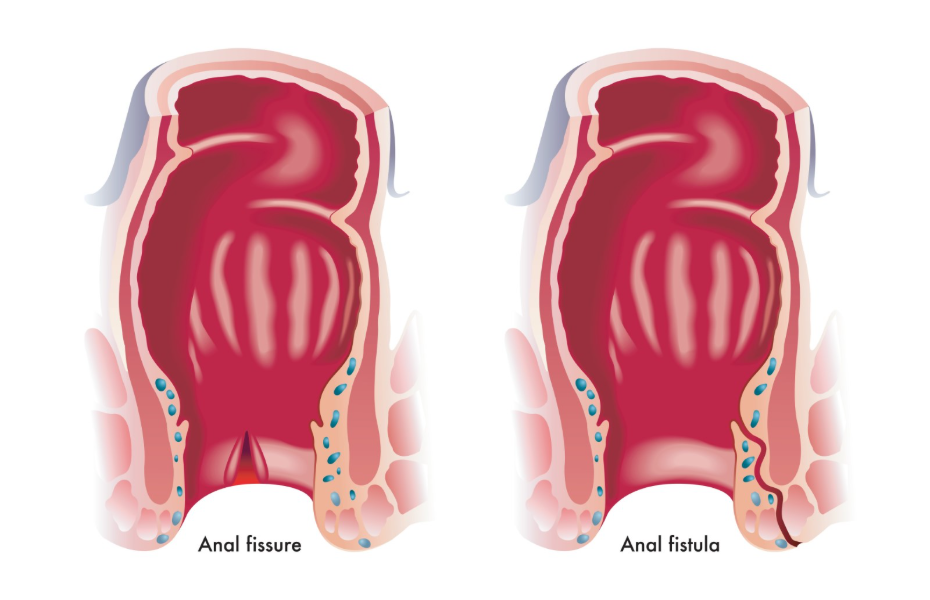
While rare, a fissure that does not heal can become infected, potentially leading to the formation of a perianal abscess or an anal fistula. Because an anal fissure is an open wound in an area naturally populated by bacteria, there is a constant risk of pathogens entering the deeper tissues. If bacteria become trapped in the tear or in one of the anal glands located near the fissure, a collection of pus, known as an abscess, may form.
An abscess typically presents as a hot, hard, and extremely painful lump that may be accompanied by a fever or general malaise. If an abscess is left untreated, it may eventually burst or be surgically drained, which can lead to the development of an anal fistula. A fistula is a small tunnel that connects the anal canal to the surface of the skin. Both abscesses and fistulas represent significant clinical complications that require surgical intervention and a much longer recovery period than a simple fissure.
Recurrence and Long Term Anal Stenosis
Leaving a fissure to heal and re-tear repeatedly can result in permanent scarring of the anal canal, which may lead to a narrowing of the opening known as stenosis. Every time the skin tears and begins to heal, the body produces scar tissue (fibrosis). Unlike the healthy, elastic mucosal lining of the anal canal, scar tissue is rigid and does not stretch easily during bowel movements.
If multiple episodes of tearing occur over several years, the accumulation of scar tissue can reduce the overall diameter of the anal canal. This narrowing makes the passage of stool even more difficult and increases the likelihood of further injury, creating a self-reinforcing cycle of trauma. In severe cases of stenosis, the anal opening loses the flexibility required for normal function, which may eventually require surgical dilation or corrective procedures to restore an adequate opening for the passage of waste.
Comparison of Acute and Chronic Features
The following table distinguishes between the characteristics of a newly formed fissure and one that has developed complications due to a lack of treatment.
| Feature | Acute Anal Fissure | Chronic/Untreated Fissure |
| Duration | Under 6 weeks | Over 6 weeks |
| Pain Pattern | Sharp sting during pooing | Sharp sting followed by long throb |
| Visual Appearance | Shallow, fresh crack | Deep tear with visible muscle fibres |
| Associated Lumps | None | Sentinel skin tags (sentinel piles) |
| Tissue State | Flexible mucosal lining | Fibrous edges and scar tissue |
| Healing Prospect | High with diet and water | Low without medicated intervention |
The Impact on Quality of Life and Bowel Habits
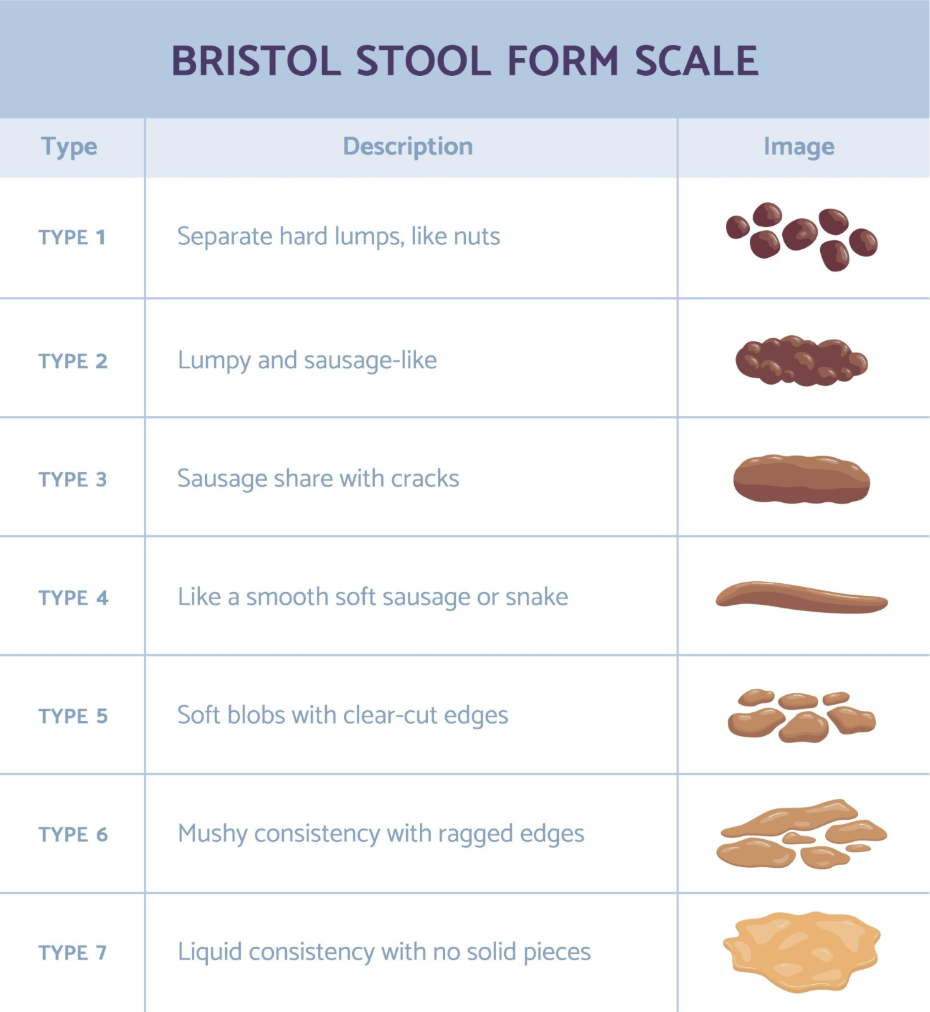
One of the most significant complications of an untreated fissure is the secondary impact on a person’s bowel habits and psychological wellbeing. Because the pain of passing stool is so intense, many individuals subconsciously or intentionally delay going to the toilet. This “toilet avoidance” causes the stool to remain in the colon for longer, where more water is reabsorbed, leading to even harder stools.
It is essential to seek medical advice if you notice bright red blood when you have a bowel movement or if the pain in your anal area is persistent. When the person eventually does have a bowel movement, the larger and harder stool causes more severe tearing and pain than before. This cycle can lead to chronic constipation and significant anxiety regarding basic bodily functions. Over time, the constant fear of pain can affect social activities, work attendance, and general quality of life, illustrating that the complications of a fissure are not purely physical.
Conclusion
Leaving an anal fissure untreated can lead to chronic pain, permanent structural changes like skin tags, and a heightened risk of localised infections. The persistent cycle of muscle spasms and restricted blood flow is the primary reason why these tears fail to heal without clinical intervention. Addressing the condition early through soft stools and proper hygiene can prevent more serious issues such as abscesses or the development of scar tissue. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Can an anal fissure turn into cancer?
There is no evidence that an anal fissure can turn into cancer, but symptoms like bleeding must be evaluated to ensure they are not caused by other conditions.
Will an untreated fissure eventually heal on its own?
While some small acute fissures heal, those that have become chronic rarely heal without specific treatments to relax the anal muscles.
What is a sentinel pile?
A sentinel pile is a small skin tag that forms at the base of a chronic fissure due to long term inflammation and the body’s attempt to protect the area.
Is it normal for a fissure to bleed every time I go to the toilet?
Frequent spotting is common with an untreated fissure, but persistent bleeding should always be reviewed by a healthcare professional to confirm the source.
Can an untreated fissure cause a fever?
A simple fissure does not cause a fever; if you have anal pain and a fever, it may indicate a perianal abscess that requires urgent assessment.
How does scar tissue affect future bowel movements?
Scar tissue is less elastic than normal skin, meaning it can tear more easily in the future or cause a narrowing of the anal canal.
Why does my untreated fissure only hurt sometimes?
The pain is often linked to stool consistency; if you are constipated, the tear is reopened, but if stools are soft, you may have temporary relief.
Authority Snapshot (E-E-A-T)
This medical education content provides accurate, evidence-based information regarding the potential complications of anal fissures for the UK public. The material is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information provided is strictly aligned with the clinical standards and diagnostic pathways provided by the NHS and the National Institute for Health and Care Excellence (NICE).
