


Warning signs that a brain tumour is worsening usually manifest as new or progressive neurological deficits that indicate increasing pressure within the skull or the involvement of new areas of brain tissue. In the United Kingdom, the NHS emphasizes the importance of symptom monitoring as part of a structured long-term care plan for anyone diagnosed with a brain tumour. Clinical teams use these observations alongside regular neuroimaging to determine if a change in management is required. While some symptoms may be side effects of treatment, a pattern of worsening signs often warrants an urgent clinical review by a specialist multidisciplinary team. The UK healthcare system follows evidence-based protocols established by NICE to ensure that patients and their families can identify red-flag symptoms promptly and safely. Understanding these clinical indicators allows for more effective communication with healthcare providers and ensures that interventions are implemented at the earliest possible stage. This article explores the primary categories of worsening symptoms, the significance of intracranial pressure, and the integrated support framework provided within the UK to manage neurological health.
What We’ll Discuss in This Article
- Changes in headache patterns and signs of increased intracranial pressure.
- The clinical significance of new or changing seizure activity.
- Progressive physical weakness and its relationship to tumour location.
- Cognitive and behavioural shifts that indicate neurological change.
- Visual and sensory disturbances as indicators of tumour growth.
- How the NHS coordinates urgent reviews for worsening symptoms.
Changes in Headache Patterns and Intracranial Pressure
A significant warning sign that a brain tumour may be worsening is a change in the frequency, intensity, or nature of headaches, particularly those caused by increased intracranial pressure. These headaches are often distinctive because they tend to be most severe in the morning and may improve slightly after the person has been upright for several hours. The NHS states that a brain tumour can cause a headache that is often worse in the morning and when coughing, sneezing or bending down.
In the United Kingdom, clinicians look for “progressive” headaches, meaning those that steadily become more painful or frequent over several days or weeks. If a headache is accompanied by persistent nausea, vomiting, or a feeling of drowsiness, it suggests that the mass or surrounding swelling is impacting the brain’s fluid balance. Unlike standard tension headaches, these are often deep and throbbing. During clinical reviews, specialist nurses will ask about these specific patterns to determine if an urgent MRI scan is needed to check the stability of the tumour site. Identifying these shifts in pain early allows the medical team to use medications like steroids to reduce swelling and alleviate pressure before symptoms become more severe.
New or Changing Seizure Activity
The development of new seizures or a significant change in the pattern of existing seizures is a primary clinical indicator that a brain tumour may be changing or putting pressure on new areas of the brain. Seizures occur because the tumour or the swelling around it disrupts the normal electrical signals between nerve cells. NICE clinical guidelines for brain tumours indicate that any new or worsening neurological deficit, including seizures, should be investigated promptly by a specialist team.
| Seizure Feature | Sign of Potential Worsening | Clinical Action in UK |
| Frequency | Episodes becoming more common. | Review of anti-epileptic medication. |
| Nature | Change from focal to generalised. | Urgent neuroimaging usually requested. |
| Duration | Longer recovery or “post-ictal” phase. | Assessment of intracranial pressure. |
| New Types | First-time seizure in a stable patient. | Priority multidisciplinary team review. |
In the United Kingdom, patients are encouraged to maintain a seizure diary to document these changes accurately. A sudden “cluster” of seizures or a first-time seizure after a long period of stability is viewed as a red-flag sign by neuro-oncologists. While seizures can sometimes be caused by treatment-related scar tissue, the clinical priority is always to rule out tumour activity. The NHS provides integrated support from epilepsy specialists to help manage these episodes while the primary medical team investigates the underlying cause. Monitoring these electrical shifts is essential for maintaining patient safety and adjusting the long-term management strategy effectively.
Progressive Physical Weakness and Coordination Loss
Progressive physical weakness, particularly when it affects only one side of the body, is a common sign that a brain tumour is impacting the motor pathways or the cerebellum. This may manifest as a heaviness in a limb, a tendency to trip, or a sudden loss of coordination in the hands. Unlike acute injuries, this weakness typically develops gradually, becoming more noticeable over the course of several days.
In the United Kingdom, physiotherapists and specialist nurses perform regular functional assessments to monitor these changes. If a patient who was previously mobile begins to require significant assistance or experiences “foot drop,” it indicates a shift in neurological health. The location of the tumour often dictates which side of the body is affected; for example, a tumour on the right side of the brain typically causes weakness on the left side of the body. Documenting these physical changes helps the multidisciplinary team determine if the tumour is involving new areas of the motor cortex. The UK healthcare framework ensures that these functional shifts are addressed through a combination of medical intervention and intensive neurorehabilitation to preserve independence for as long as possible.
Cognitive Shifts and Behavioural Changes
Worsening of a brain tumour can lead to noticeable shifts in cognitive function, memory, and social behaviour, particularly if the mass is located in the frontal or temporal lobes. These changes might include increased confusion, difficulty finding words, or a significant shift in temperament that is out of character for the individual. The GOV.UK health pages provide clinical profiles indicating that personality and cognitive changes are recognised indicators for urgent review in cancer service standards.
Common cognitive warning signs in the UK include:
- Difficulty with Language: Struggling to understand others or being unable to name common objects.
- Memory Loss: A sudden inability to remember recent events or follow familiar routines.
- Reduced Concentration: Becoming easily distracted or unable to complete simple tasks.
- Behavioural Shifts: Increased irritability, apathy, or a loss of social inhibition.
These “hidden” symptoms are often first noticed by family members or carers rather than the patient themselves. In the United Kingdom, neuropsychologists provide specialist assessments to measure these changes objectively. Because these symptoms can also be caused by medication side effects or infection, a comprehensive clinical review is necessary. However, when these shifts are progressive and accompanied by other neurological signs, they serve as a vital indicator that the tumour or its associated swelling may be increasing, requiring a prompt review of the current management plan.
Visual Disturbances and Sensory Changes
Visual disturbances, such as double vision, loss of peripheral vision, or sudden blurring, can indicate that a brain tumour is worsening and affecting the visual pathways or increasing pressure on the optic nerves. These changes may occur gradually or become apparent during specific activities like reading or navigating a busy room.
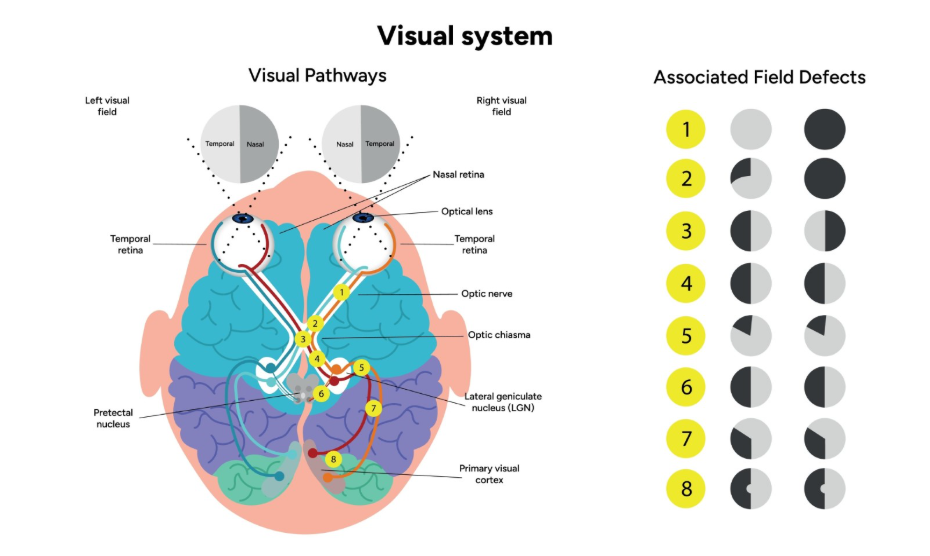
Patients in the United Kingdom are often advised to have regular eye tests, as opticians can detect swelling behind the eye even if the patient’s vision feels normal. Other sensory changes can include numbness, a “pins and needles” sensation, or a loss of temperature awareness in specific parts of the body. In the UK healthcare system, these sensory shifts are mapped carefully by neurologists to see if they correspond with the known tumour site. If a person experiences a sudden “curtain” falling over their vision or a significant loss of field, it is treated as a clinical priority. Monitoring these sensory inputs is a critical part of the long-term surveillance pathway, as the eyes and skin provide a direct “map” of the brain’s functional health.
Coordinating Urgent Reviews in the NHS
The United Kingdom provides a structured framework for coordinating urgent reviews when warning signs of a worsening tumour are identified. This system ensures that patients move quickly from a community or home setting into a specialist clinical environment for diagnostic imaging and assessment.
The UK urgent review process involves:
- Triage by Specialist Nurse: The key worker assesses the reported symptoms to determine urgency.
- Priority MRI Imaging: Scheduling a scan within days to check for tumour growth or swelling.
- MDT Discussion: A multidisciplinary team of surgeons and oncologists reviewing the latest data.
- Management Adjustment: Implementing new treatments like steroids or further surgery promptly.
This integrated safety net relies on open communication between the patient and their medical team. In the UK, the focus is on “safety-netting,” where patients are given clear instructions on who to contact if they notice any specific changes. This proactive approach aims to identify issues before they become emergency situations. By utilizing this framework, the NHS provides a continuous link between regular monitoring and acute intervention, ensuring that any worsening of the condition is addressed with the full expertise of the neuro-oncology service.
Conclusion
There are several clinical warning signs that a brain tumour may be worsening, including progressive headaches, new or changing seizures, and shifts in physical or cognitive function. In the UK, the NHS uses these indicators as triggers for urgent specialist reviews and priority neuroimaging. Monitoring these changes through a symptom diary is a vital part of long-term care, helping the multidisciplinary team adjust treatments such as steroids or surgery. While some symptoms may relate to treatment side effects, progressive neurological deficits always require a medical assessment. Following the structured surveillance pathway ensures that any biological change is identified and managed as quickly as possible. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Is every new headache a sign that the tumour is growing?
No; many headaches are caused by stress, dehydration, or medications, but a persistent, worsening, or morning headache should be reported.
What should I do if my speech suddenly becomes slurred?
You should contact your specialist nurse or the 24-hour oncology help line provided by your hospital for an urgent assessment.
Can a change in mood be the only sign of worsening?
While rare, significant and progressive changes in personality or behaviour can indicate a shift in neurological health and warrant a review.
How quickly will the NHS see me if I report a red-flag symptom?
The UK healthcare system aims to triage and review priority cases rapidly, often arranging a scan or consultation within a few days.
Do steroids always help when symptoms worsen?
Steroids are very effective at reducing the swelling around a tumour, which often improves symptoms even if the tumour itself hasn’t shrunk.
Could my worsening symptoms be caused by an infection?
Yes; infections like a UTI can cause increased confusion or weakness in brain tumour patients, which is why a full clinical review is necessary.
How can I tell the difference between a seizure and a faint?
A seizure often involves rhythmic movements or a period of confusion afterward; your medical team will use your diary to make this distinction.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the warning signs of a worsening brain tumour, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery, emergency medicine, and psychiatry. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


