


Scientific evidence suggests a complex relationship between hormones and certain types of brain tumours, particularly those arising from the pituitary gland or meninges. In the United Kingdom, medical researchers study how hormonal fluctuations and endocrine health influence the growth of specific tumours, such as meningiomas or pituitary adenomas. While most brain tumours are not directly caused by hormonal imbalances, the brain’s endocrine system plays a vital role in regulating the environment in which these tumours develop. The NHS and NICE provide evidence-led guidance to help patients understand these biological links while focusing on established risk factors like age and genetics. By integrating neuro-oncology with endocrinology, the UK healthcare system ensures a comprehensive approach to managing tumours that interact with the body’s chemical messengers. This article explores the clinical connection between hormones and different tumour types, the impact of reproductive history, and the integrated support framework provided within the UK to manage these complex neurological conditions.
What We’ll Discuss in This Article
- The role of the pituitary gland in hormonal tumour development.
- The relationship between sex hormones and meningioma growth.
- How pregnancy and reproductive history influence neurological risk.
- Clinical evidence regarding hormone replacement therapy (HRT).
- Managing hormonal symptoms through integrated NHS specialist care.
- Recognised risk factors and the importance of clinical surveillance.
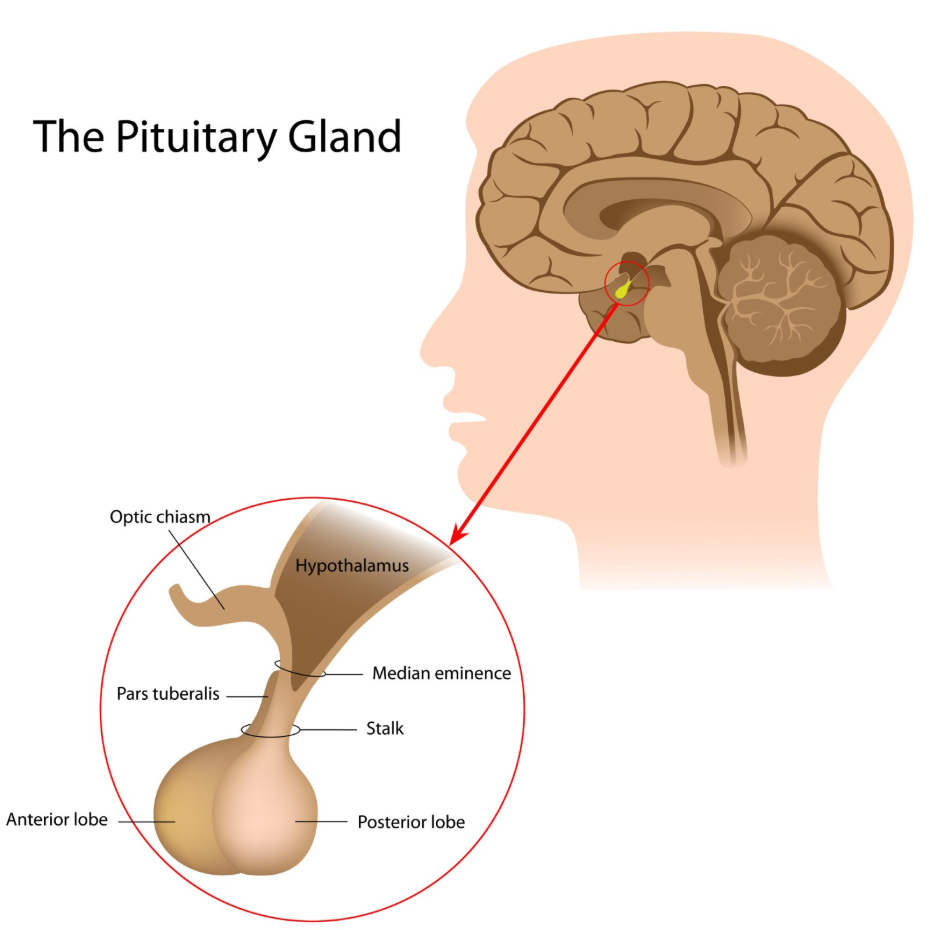
Pituitary Gland Function and Adenoma Development
The pituitary gland is a master control centre for the body’s hormones, and tumours developing in this region are almost always linked to changes in hormonal production or regulation. These growths, known as pituitary adenomas, can cause the gland to produce too much of a specific hormone or prevent it from producing enough. The NHS states that tumours of the pituitary gland are quite common and can cause symptoms by pressing on nearby nerves or by changing hormone levels.
In the United Kingdom, pituitary adenomas are classified as functioning or non-functioning depending on whether they secrete excess hormones. Functioning tumours can lead to conditions such as acromegaly or Cushing’s syndrome, which have widespread effects on the body’s metabolism and physical structure. Because these tumours are located near the optic nerves, they can also impact vision. UK clinical teams include endocrinologists who work alongside neurosurgeons to manage these hormonal imbalances through medication, surgery, or radiotherapy. This integrated approach ensures that the systemic effects of the tumour are addressed simultaneously with the physical mass.
Sex Hormones and the Growth of Meningiomas
There is a recognised clinical link between female sex hormones, such as progesterone and oestrogen, and the development or growth rate of meningiomas. Meningiomas are tumours that grow from the protective membranes surrounding the brain, and they are significantly more common in women than in men. NICE clinical guidelines for brain tumours indicate that hormonal receptors within meningioma cells can influence how the tumour behaves and its potential for growth during different life stages.
Medical research in the United Kingdom has found that many meningioma cells contain receptors for progesterone, meaning the hormone can act as a signal for the cells to divide. This relationship explains why some meningiomas are identified or show changes during periods of significant hormonal shift. However, it is important to note that hormones are typically considered a factor that influences the growth of an existing tumour rather than the primary cause of the initial mutation. In the UK, specialists monitor these tumours closely in female patients, particularly if they are considering treatments that significantly alter hormone levels. Understanding this biological link allows for more personalised management strategies that consider the patient’s hormonal profile alongside their neurological health.
Pregnancy and Reproductive History Factors
Pregnancy involves profound hormonal changes that can occasionally impact the clinical presentation or growth of certain brain tumours, particularly meningiomas and pituitary adenomas. The high levels of progesterone and oestrogen during pregnancy can, in some cases, cause a previously dormant or slow-growing tumour to increase in size or become symptomatic.
| Factor | Potential Impact | UK Clinical Consideration |
| Pregnancy | Increased growth rate of meningiomas. | Monitoring of neurological symptoms. |
| Puberty | Shifts in pituitary tumour activity. | Endocrine and growth surveillance. |
| Menopause | Potential stabilisation of some tumours. | Review of hormone replacement needs. |
| Parity | Complex links to overall life risk. | Research shows inconsistent associations. |
In the United Kingdom, if a brain tumour is identified during pregnancy, the multidisciplinary team carefully balances the health of the mother and the baby. While the hormones of pregnancy can stimulate growth, many tumours remain stable and do not require immediate intervention. Following delivery, when hormone levels return to their baseline, some tumours may even show a slight reduction in size or a slowing of growth. This nuanced relationship is managed through regular MRI surveillance and clinical reviews. The focus of UK healthcare is to provide safe, evidence-based care that acknowledges the impact of reproductive biology on neurological stability.
Hormone Replacement Therapy and Neurological Risk
The use of Hormone Replacement Therapy (HRT) and its link to brain tumour risk is a subject of ongoing clinical study in the United Kingdom, with evidence suggesting a small increase in the risk of being diagnosed with a meningioma. Large-scale observational studies have indicated that long-term use of certain types of hormone therapy may correlate with a higher incidence of these specific slow-growing tumours. The GOV.UK health pages provide clinical profiles and safety updates indicating that the risks and benefits of HRT should be balanced on an individual basis, especially for those with a history of meningioma.
Current UK medical advice does not suggest that HRT causes high-grade or malignant brain tumours. For most women, the benefits of HRT in managing menopausal symptoms and protecting bone health outweigh the small statistical risk of a meningioma. However, for individuals who have already been diagnosed with a meningioma, UK consultants may advise caution or suggest alternative treatments to manage menopausal symptoms. This clinical decision-making is highly individualised and based on the specific type and location of the tumour. By discussing these risks with a GP or specialist, patients in the UK can make informed choices about their hormonal health.
Integrated NHS Specialist Care and Monitoring
Managing tumours with a hormonal link requires an integrated approach that combines neurosurgical expertise with specialist endocrinology. In the United Kingdom, the NHS provides multidisciplinary teams (MDTs) that ensure all aspects of a patient’s hormonal and neurological health are monitored concurrently.
The UK integrated care framework involves:
- Endocrinology Reviews: Monitoring hormone levels and managing replacement therapies.
- Neurosurgical Surveillance: Regular MRI scans to track the physical size of the tumour.
- Specialist Nurse Support: Providing a link between different medical specialities.
- Visual Field Testing: Checking for impact on sight, particularly with pituitary tumours.
This coordinated system is essential for patients with functioning pituitary tumours, where the primary symptoms may be metabolic rather than neurological. In the UK, the focus is on achieving biochemical control of hormone levels while ensuring the tumour remains stable. Accessing these services through a specialist centre ensures that the patient benefits from the latest research and evidence-based protocols. This professional safety net provides patients with the comprehensive oversight needed to manage the long-term implications of hormonally active brain tumours.
Conclusion
A link exists between hormones and certain brain tumours, specifically pituitary adenomas and meningiomas, which can be influenced by changes in the body’s chemical messengers. In the UK, the NHS manages these conditions through integrated teams of neurologists and endocrinologists to ensure both the mass and the hormonal balance are addressed. While pregnancy and certain hormone therapies may influence tumour growth, they are rarely considered the primary cause of the condition. Most other types of brain tumours do not have a proven hormonal connection and are managed through standard oncological pathways. Consistent monitoring through the multidisciplinary team remains the most effective way to manage these complex health issues. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
Does the contraceptive pill increase my risk of a brain tumour?
Current UK evidence does not show a significant link between the use of the combined oral contraceptive pill and an increased risk of brain tumours.
Can a brain tumour cause me to stop having periods?
Yes; tumours affecting the pituitary gland can disrupt the hormones that regulate the menstrual cycle, leading to changes or cessation of periods.
Is HRT safe if I have a family history of brain tumours?
Most brain tumours are not hereditary; for most people, a family history does not change the safety profile of HRT regarding neurological risk.
Why does pregnancy make some tumours grow?
The high levels of progesterone during pregnancy can act on receptors in some tumour cells, stimulating them to divide more rapidly.
Will my hormone levels return to normal after the tumour is removed?
Many patients require long-term hormone replacement therapy if the pituitary gland was damaged by the tumour or its treatment.
Are men affected by hormonal brain tumours?
Yes; men can develop pituitary adenomas that affect testosterone or prolactin levels, requiring the same integrated endocrine and neurological care.
Can stress hormones cause a brain tumour?
No; there is no scientific evidence that cortisol or other stress-related hormones cause the genetic mutations that lead to brain tumours.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the link between hormones and brain tumours, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Rebecca Fernandez, a UK-trained physician with experience in general surgery, cardiology, and emergency medicine. All information follows current UK public health protocols to ensure clinical accuracy and patient safety.


