

Jaundice can return after it has been treated if the underlying medical cause remains unresolved, if a chronic liver condition experiences a flare-up, or if new physical obstructions develop within the biliary system. Because jaundice is a visible symptom of elevated bilirubin levels rather than a standalone disease, its recurrence indicates that the body’s ability to process and excrete this yellow pigment has been compromised once again. In the United Kingdom, healthcare professionals monitor for recurrent jaundice to identify potential issues such as new gallstones, the progression of chronic hepatitis, or the impact of certain medications on liver function. While initial treatment may successfully clear the pigment from the skin and eyes, long-term health depends on the stability of the liver and the clear passage of the bile ducts. Understanding the factors that contribute to the return of jaundice is essential for patients to manage their health proactively and recognise when further clinical investigation is necessary. Because the liver serves as the body’s primary filtration hub, any return of yellowing serves as a critical signal that the organ is under metabolic or physical stress.
What We’ll Discuss in This Article
- The biological mechanisms that allow bilirubin levels to rise again after treatment.
- How chronic liver conditions like cirrhosis can cause fluctuating jaundice.
- The risk of recurrent gallstones and their impact on the bile ducts.
- The role of medication and toxins in triggering a return of symptoms.
- Clinical indicators that differentiate between a new issue and a relapse.
- UK healthcare protocols for managing and monitoring recurrent jaundice.
The Relationship Between Underlying Causes and Recurrence
Jaundice returns when the initial treatment only addressed the immediate symptom or a temporary blockage without resolving the long-term vulnerability of the liver or biliary tree. The NHS states that jaundice is often a sign of an underlying liver problem, and if that problem is not fully managed, the symptoms can return. For example, if a patient is treated for a blocked bile duct but the source of the blockage, such as the gallbladder, remains in place, new stones can easily form and migrate into the duct again. Similarly, if jaundice was caused by inflammation that has only partially subsided, any new insult to the liver can cause bilirubin levels to spike once more. In the UK, clinicians categorise recurrent jaundice based on whether the issue is pre-hepatic, intra-hepatic, or post-hepatic to determine the most effective secondary management plan.
Chronic Liver Disease and Fluctuating Jaundice
Chronic liver conditions, such as cirrhosis or autoimmune hepatitis, often lead to fluctuating jaundice where the yellowing of the eyes and skin may appear to resolve before returning during periods of illness or stress. In these cases, the liver has a reduced functional reserve due to permanent scarring or ongoing inflammation.
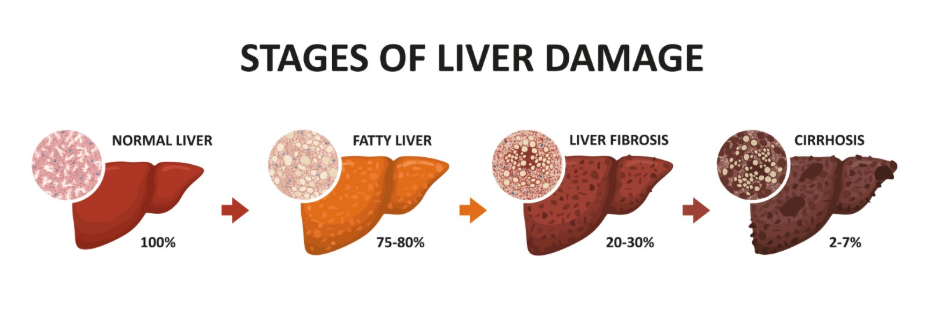
When the body is under stress perhaps due to a minor infection, dehydration, or a change in medication the liver may reach a breaking point where it can no longer process bilirubin effectively. This leads to “decompensation,” where symptoms like jaundice, fatigue, and fluid retention reappear. NICE clinical guidelines for the management of cirrhosis emphasise that the return of jaundice in a patient with known liver disease is a significant clinical marker that requires urgent review to prevent further organ failure.
| Stage of Liver Health | Bilirubin Processing | Jaundice Risk |
| Healthy Liver | Efficiently processed and excreted. | Very Low |
| Compensated Cirrhosis | Processed adequately despite scarring. | Intermittent/Low |
| Decompensated Cirrhosis | Processing pathways are overwhelmed. | High/Persistent |
Recurrent Biliary Obstruction and Gallstones
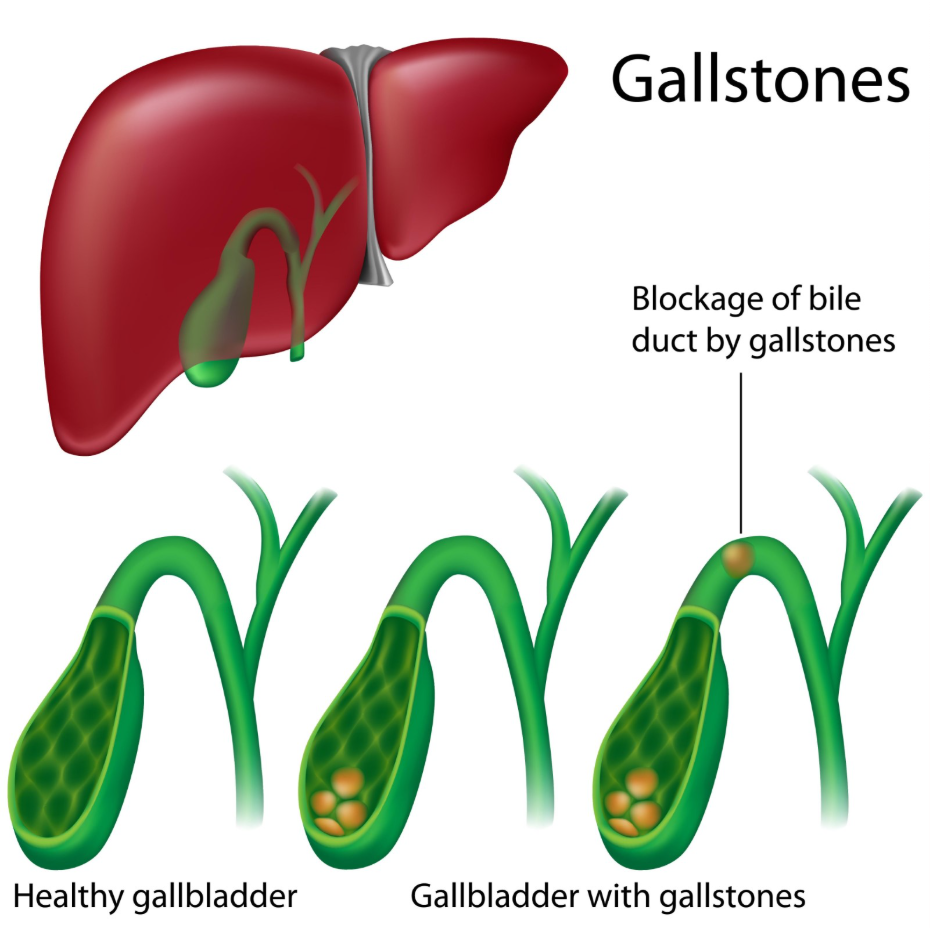
The return of jaundice is frequently linked to the recurrence of gallstones in individuals who have not had their gallbladder removed or who develop stones directly within the bile ducts. Even if a stone was successfully removed via a procedure like an ERCP, the gallbladder remains a reservoir where new stones can be produced.
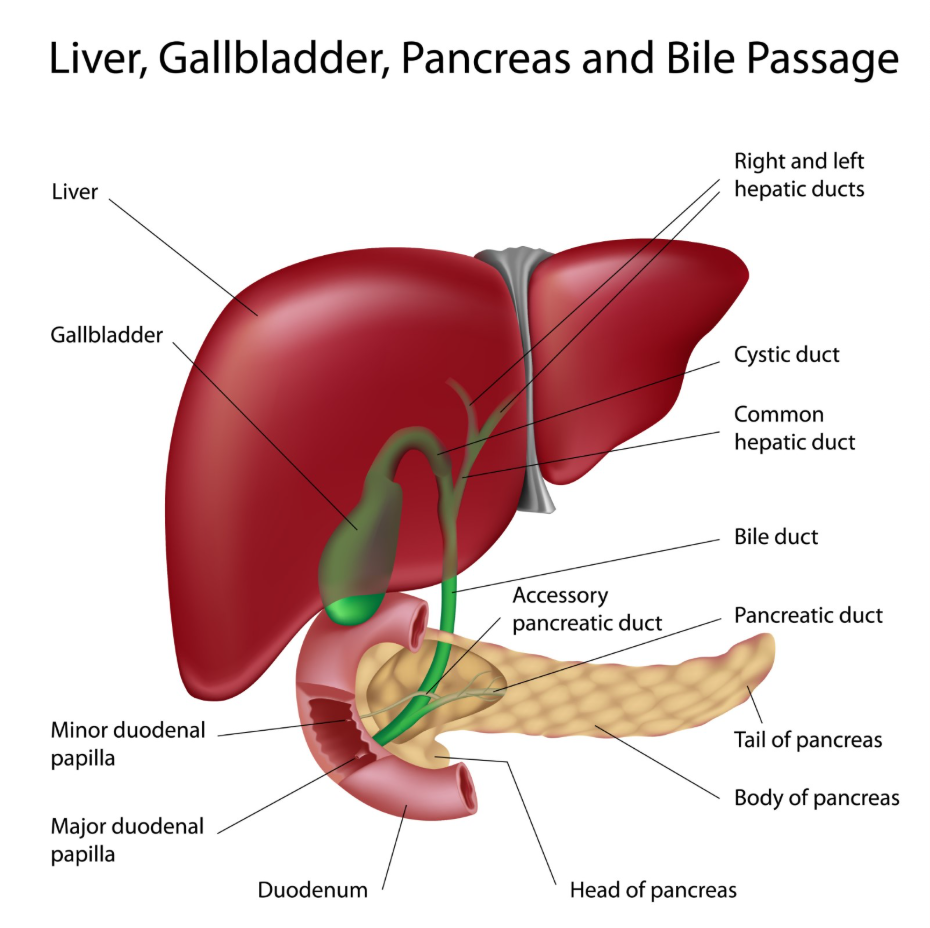
If a new stone migrates and blocks the common bile duct, the flow of bile is interrupted, and jaundice will return rapidly, often accompanied by dark urine and pale stools. According to the GOV.UK health profiles, gallstones are a leading cause of hospital readmissions for jaundice in the UK, highlighting the importance of definitive surgical management. In some cases, the bile ducts themselves may narrow due to previous inflammation or surgery (strictures), making it easier for even small amounts of debris to cause a significant blockage and a return of symptoms.
Impact of Medications and Environmental Toxins
Certain medications and toxins can trigger a return of jaundice by causing direct injury to the liver cells or by interfering with the organ’s internal transport systems. This is particularly common in individuals who have a pre-existing liver sensitivity or who are prescribed multiple medications that are processed through similar metabolic pathways. Drug-induced liver injury (DILI) can manifest as jaundice weeks or even months after starting a new therapeutic agent.
Environmental factors, such as excessive alcohol consumption or exposure to industrial chemicals, can also cause the liver to become inflamed again. In the UK, a thorough review of a patient’s recent chemical and supplement intake is a standard part of investigating recurrent jaundice. If the liver was already weakened by a previous episode, it may be more susceptible to secondary injury from substances that a healthy liver would otherwise manage without difficulty.
Identifying New Symptoms versus Relapse
When jaundice returns, UK healthcare providers must determine if the patient is experiencing a relapse of the original condition or if a entirely new medical issue has developed. A relapse suggests that the primary treatment was insufficient or that the underlying disease is progressing. A new issue, such as a viral infection occurring in someone with known gallstones, requires a different diagnostic focus.
Clinicians look at the pattern of blood results specifically the ratio of liver enzymes to differentiate between these possibilities. For example, if the enzymes related to the bile ducts (ALP) are rising while the liver cell enzymes (ALT) remain stable, it suggests a new mechanical obstruction rather than a flare-up of hepatitis. This detailed biochemical analysis ensures that the patient does not receive unnecessary treatment for the wrong condition and that any serious new developments are caught early.
Clinical Monitoring and Long-Term Surveillance
The prevention and management of recurrent jaundice in the UK involve consistent clinical monitoring and long-term surveillance programmes for those at high risk. For patients with chronic liver disease, this includes regular blood tests to track bilirubin and albumin levels, alongside ultrasound scans to monitor for structural changes or new growths.
By establishing a baseline for each patient, the multidisciplinary healthcare team can identify even subtle rises in bilirubin before the yellowing becomes visible to the eye. This proactive approach allows for earlier intervention, such as adjusting medications or performing a minor procedure to keep a bile duct open. Patients are also encouraged to participate in lifestyle management, such as alcohol cessation and weight control, to reduce the overall metabolic burden on the liver and minimise the chances of jaundice returning.
Conclusion
Jaundice can return after treatment if the underlying cause is chronic, if new obstructions form, or if the liver is subjected to new toxic or inflammatory stress. The reappearance of yellowing in the skin and eyes is an important clinical signal that the body’s bilirubin processing system is once again failing to keep up with metabolic demands. In the UK, managing recurrence involves a combination of blood monitoring, diagnostic imaging, and identifying potential new triggers. Maintaining a long-term care plan and adhering to lifestyle recommendations are the most effective ways to support liver health and prevent symptoms from returning. If you experience severe, sudden, or worsening symptoms, call 999 immediately.
If my gallbladder was removed, can my jaundice still return?
Yes, while less common, stones can occasionally form directly in the bile ducts, or other issues like liver inflammation can still cause jaundice.
Can a minor cold or flu make my jaundice come back?
In someone with a pre-existing liver condition like Gilbert’s syndrome or cirrhosis, the stress of a viral infection can cause a temporary rise in bilirubin.
Why did my jaundice return after I finished my antibiotics?
If the antibiotics were for a bile duct infection caused by a stone, the jaundice may return if the stone was never physically removed.
Is the return of jaundice always more serious than the first time?
Not necessarily, but it always requires a fresh medical assessment to determine if the cause is the same or something new.
Can stress at work trigger a return of jaundice?
Stress alone does not cause jaundice in a healthy liver, but it can worsen the symptoms of certain chronic liver or metabolic conditions.
How soon after treatment should I worry if I look yellow again?
Any return of yellowing should be reported to your doctor within 24 hours so they can check your bilirubin levels.
Will I need the same tests again if the jaundice returns?
Usually, yes; doctors will need new blood tests and possibly a new scan to see what has changed since your last treatment.
Authority Snapshot (E-E-A-T)
This article provides medically factual health education regarding the recurrence of jaundice, strictly aligned with NHS and NICE clinical guidelines. The content is developed by a professional medical writing team and reviewed by Dr. Stefan Petrov, a UK-trained physician with experience in general medicine, surgery, and emergency care. All information follows current UK public health protocols to ensure accuracy and patient safety.
